Coronary artery lesions can be classified by many types . The popular ones are by Ambrose and Ellis .They are adopted by ACC and SCAI .While various terms are used to describe a lesion. (diffuse, discreet , eccentric , long , tubular etc) A tandem lesion is the one which has special significance , but is not well discussed in the literature .
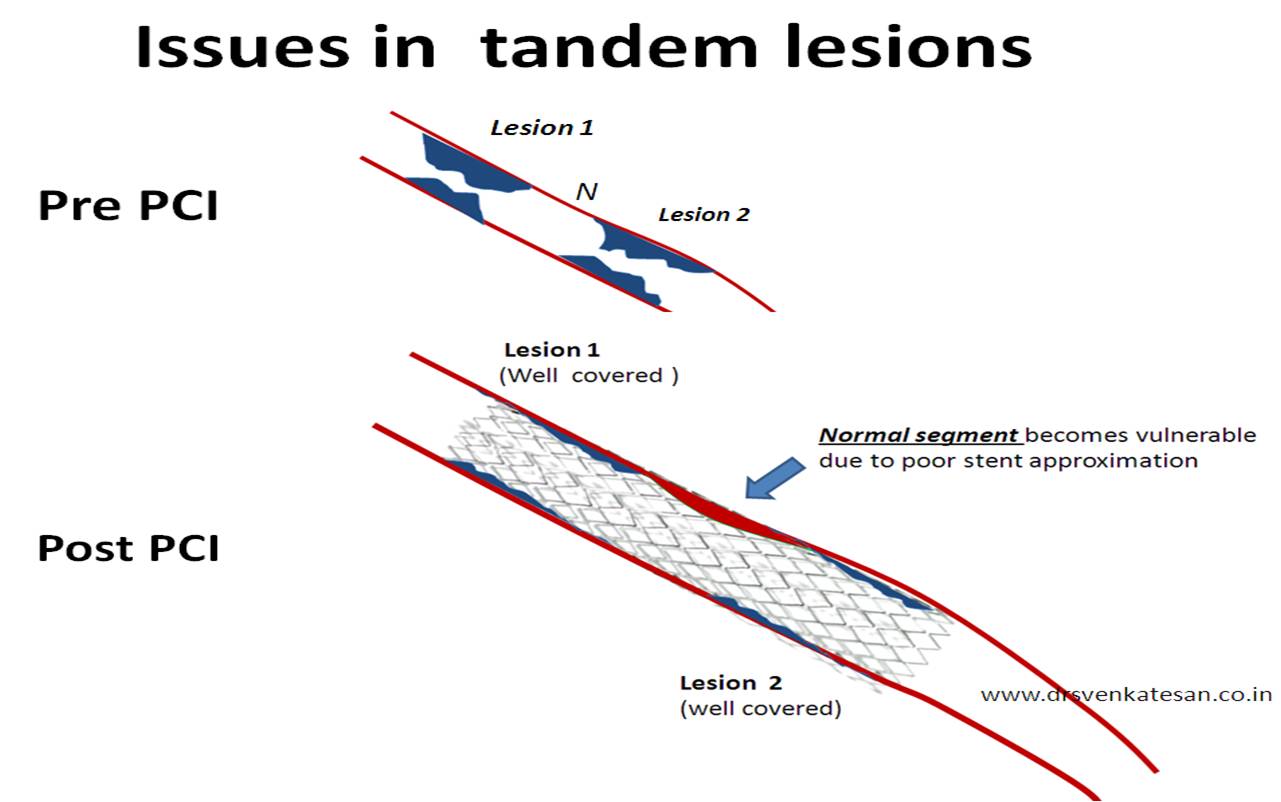
A tandem lesion is diagnosed when two lesions closely abut each other one behind the other with an intervening normal segment. (Like the bullets loaded in a tandem fashion in a gun )
Generally there will be at least few millimeters of normal intervening coronary segment.This is referred to as connecting segment.

Clinical importance of tandem lesion
Tandem lesions carry the same significance like any other lesion. But ,the primary aim is to tackle the two lesions with a single stent. We know stent edges are rheological culprits. Two stents have 4 edges. It is better to cover the tandem lesions with one long stent* even if we have a sufficient connecting segment.Geographical miss is less likely with a long stent. In the strict sense one wold require an IVUS (Intra vascular ultra sound ) to confirm the normality of the connecting segment. Tandem lesion is a marker of diffuse atherosclerosis and the connecting segments often show ectatic changes.
* This is a ironical as the conventional wisdom would tell us , lesser the metal load it is better for our coronary arteries.But once we embark on a complex intervention we just can’t restrict the use of stents. The more you put the more it will demand.There are some interventional cardiologists who convert the entire coronary artery in to a metal tube (With or without realising the consequences !)
Illusions of tandem lesion.
Many times , spiral folds from a single atherosclerotic lesion mimics a double lesion .This need to be differentiated from true tandem lesion.
What is the hemodynamic significance of tandem lesions ?
Rules of hemodynamics would dictate , in a linear and laminar flow model across a tube , immediately after an obstruction there will be a significant drop in resistance.
This forms the fundamental phenomenon within the coronary artery . This explains the biggest mystery in cardiology . . . How the TIMI flow is maintained till 90 % of the lumen is narrowed. This also explains the concept of flow limiting lesion .(Why a coronary lesion do not obstruct the flow till late stages ?)
Does this rule on hemodynamics apply in tandem lesions ?
When a lesion is followed by a lesion with little normal segment in between what happens ?
The blood gets a double jolt every time it traverses a tandem lesion. There may not be sufficient time and anatomy for the mandatory pressure drop to occur. So for a given degree of obstruction , tandem lesions is likely to be more thermodynamically significant than a single lesion.
Pressure recovery after an obstruction is also incomplete , as the forward head of blood column encounters another hurdle even before it recovers from the initial turbulence.
Which lesion is more important in tandem proximal or distal ?
The distal lesion determines the thermodynamics of proximal lesion while the distal lesion as such is less influenced by proximal.
Long lesion vs tandem lesions


Some times it may appear , it is better to have a long lesion than a two lesion in tandem. This is because the stent will approximate more evenly .Further there is less likely hood of in -stent restenosis in long lesions as the edge effect can occur right in the middle of the stent in tandem lesions .
Now it is increasingly realised, many of the sub acute thrombosis are due to po0r stent approximation in tandem lesions or long lesion.

http://www.springerlink.com/content/g063752436617n51/

http://www.ncbi.nlm.nih.gov/pubmed/8789675
Read Full Post »
 When left circumflex equals the size of left main the pattern is distinctly unusual.
When left circumflex equals the size of left main the pattern is distinctly unusual.



















{kind=link}