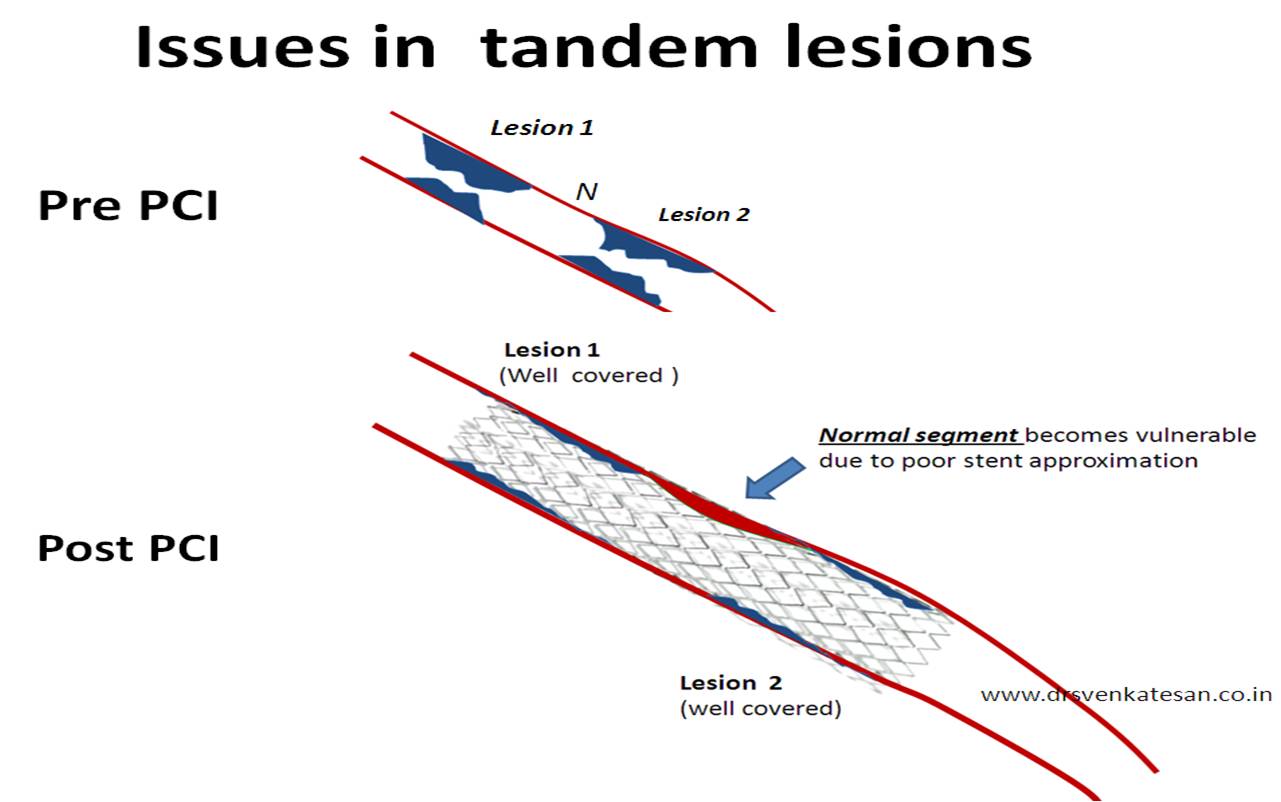
During primary PCI , the weakest link for a cardiologist is , he is never sure whether the metal jacket has covered the entire disease segment with optimal apposition . (Geographical miss is another issue !)
This is because , even though the inflation pressure is uniform within the balloon , the required apposition pressure is not the same .This is obvious as the lesion surface has a varying consistency and uneven surfaces . It is a huge guess to quantitate the relative contribution of thrombus and plaque within the 100 % occlusion that has resulted in the STEMI. Hence some areas may get over apposed and others lesser apposed. Further , the stent -vessel wall interface in all likely hood enclose a layer of clot .This is almost certain during complex primary PCI. One can imagine the sequel if this thrombus layer dissolves later ! (Edentulous stent )
It is surprising , why cardiologists has so far not thought of a self expanding stent which can snugly appose the vessel wall in this setting . The radial strength from the stored potential energy can be used up future use. This is most important in first few days following STEMI , when the coronary arterial lumen can vary depending upon the
- Vasomotor tone .
- presence of thrombus
- Plaque ploughing /milking effect
- Vascular remodeling
Cardiologists deploy a stent based on the morphology on day zero of STEMI .This may be totally irrelevant , since after a few days the lesion may change its morphology , thrombus may migrate , vascular dimension may change. In such a situation* , a self expanding stent can tackle these issues very effectively by constantly adjusting and fine tuning the luminal diameter and the apposition pressure . It does not give any chance for thrombus to form between the vessel wall and stent .
Here is a study that gives fresh insights regarding the role of self expanding stents during STEMI .


- Note the “Auto adjusting” of stent diameter in the first few days after the stent deployment, depending upon the luminal needs !

Animation
http://www.stentys.com/file_bdd/annexes/1284135580_video_stentys_en.swf
* Logically during primary PCI for STEMI , POBA and thrombus suction may be the best option in many as all stent related complication is instantly eliminated .But it is a battered concept , most of the current day cardiologists would feel guilty to come out of the cath lab without a stent in primary PCI scenario !
Final message
Self expanding stents during primary PCI : Is it a perfect solution for optimal stent apposition ?
It seems so . . . but the track record of current cardiology devices never fulfilled the initial promises !















{kind=link}