It is a 120-year challenge. Can anyone replace Rontgen’s X-ray discovered in 1895 for medical imaging? The Nobel winning Invention redefined the way we looked at our body and management of diseases for over a century. However, the fact remained it is an invasive and injuring investigation. What is the alternative for the X-radiation ?
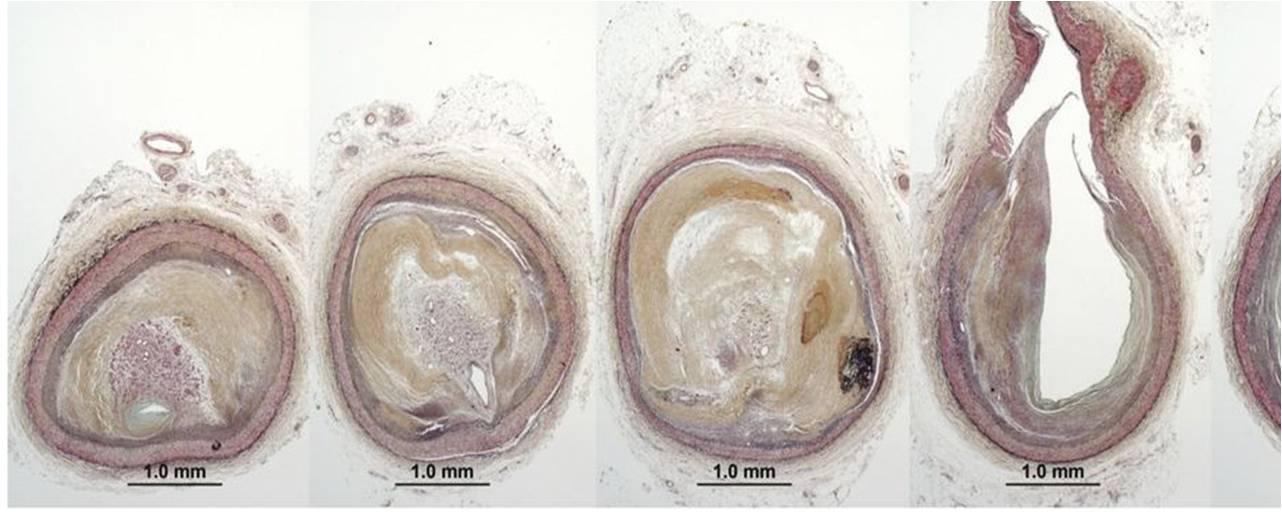
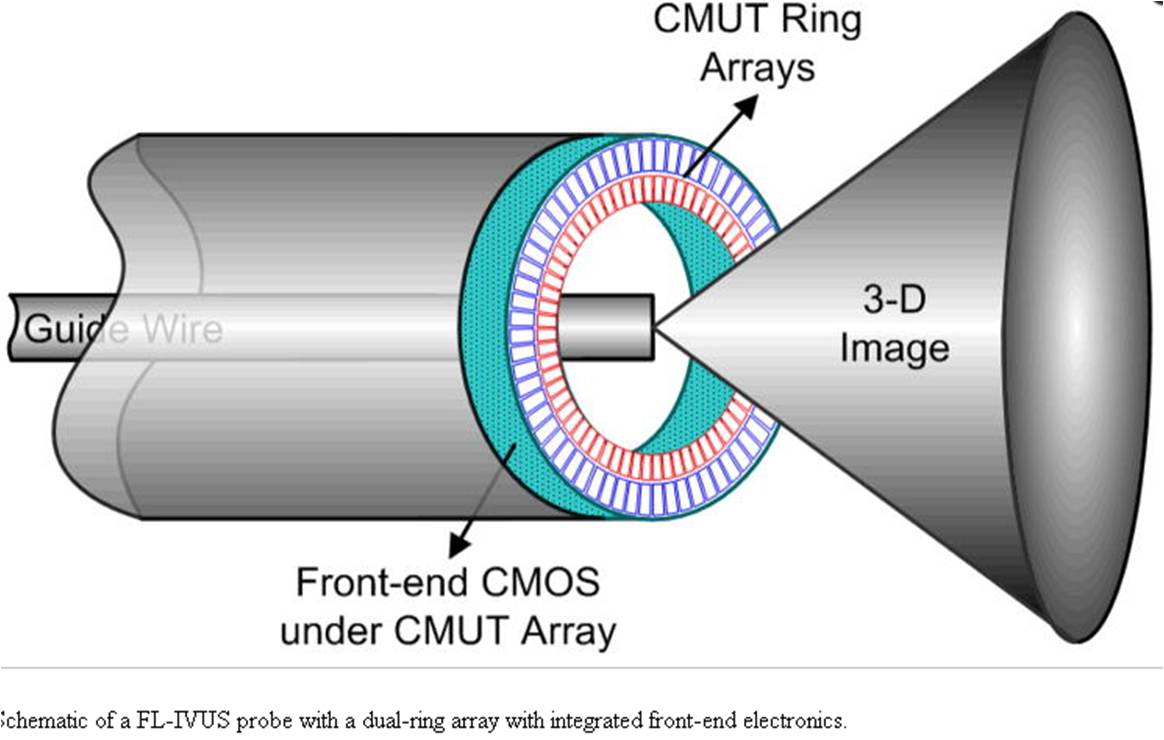
CT scan was a great invention, but it turned out to be a gigantic 360-degree clone of X-ray machine. Today’s cath lab, however sophisticated , is like spending hours together inside a hot Chernobyl coffee shop. MRI was a true game changer. With zero radiation, MRI came close in the fight with innocuous proton imaging. But for live cardiac interventions, MRI was not practical. Meanwhile, over the years, ultrasound moved up from the pelvis, abdomen, right into coronary arteries and heart. Intravascular ultrasound-based interventions are being done in coronary artery, in a few cases to avoid contrast in patients with CKD. (We call it zero-contrast IVUS-guided PCI). But, it is cumbersome and has some technical issues. Transesophageal echo (TEE) & Intracardiac echocardiography (ICE) do help us immensely in certain interventions.
Now is the era of Optics
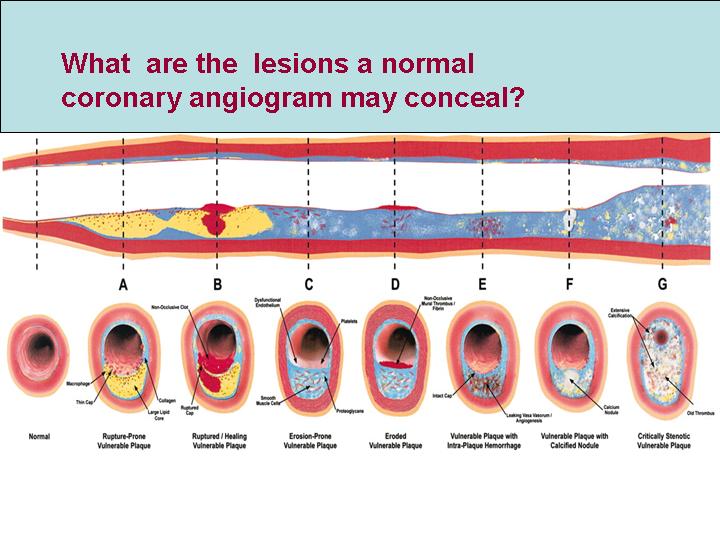
If a torch light can illuminate and give us vision in absolute darkness ,how about acquiring a deep vision with scattered light ie photons. (Jnana-Chakshush ,third eye of Hindu God Shiva ?) The concept of Optical coherence imaging came (OCT) came in .It has limited use in deep vision of coronary wall anatomy and histology. As of now it has no role to play in catheter guidance.
Here comes the real Innovation . Fibro-Optic real shape( FORS) technology , which reconstructs image from optical data, and beam live fluro- like images, in 3 dimension. May be, we may soon, say good bye to electrons, protons, and welcome these harmless photons.
This video clip shows real time Intervention using FORS in Aortic endovascular stenting
One may Imagine FORS to Electro-physiologist’s electro- anatomic mapping made with a the GPS like pad attached beneath the cath table and reconstructing anatomical Images from the dynamic signals points generated from the catheter tip.
Final message
Now, we are looking at various different modalities to image without radiation injury to the patients, and more importantly the cardiologists .
- Intra cardiac Echocardiography (ICE)
- Proton imaging (MRI)
- Electrical navigation (CARTO)
- Fibro-Optic real shape (FORS)
FORS , is the new arrival. Let us hope it stands the test of time.
.