How many times you have treated cardiac arrhythmia in both emergency & non-emergency situations?
Infinite times.
How many times did you really bother to know the mechanism of a given arrhythmia before ordering medication or shocking?
Hmm,.. let me think. (Except for AVNRT/ AVRT, and few VTs, very rarely I have worried about the mechanism !)
Why is it so? because treatment takes priority and we are able to tame the arrhythmia even without knowing the real mechanism.
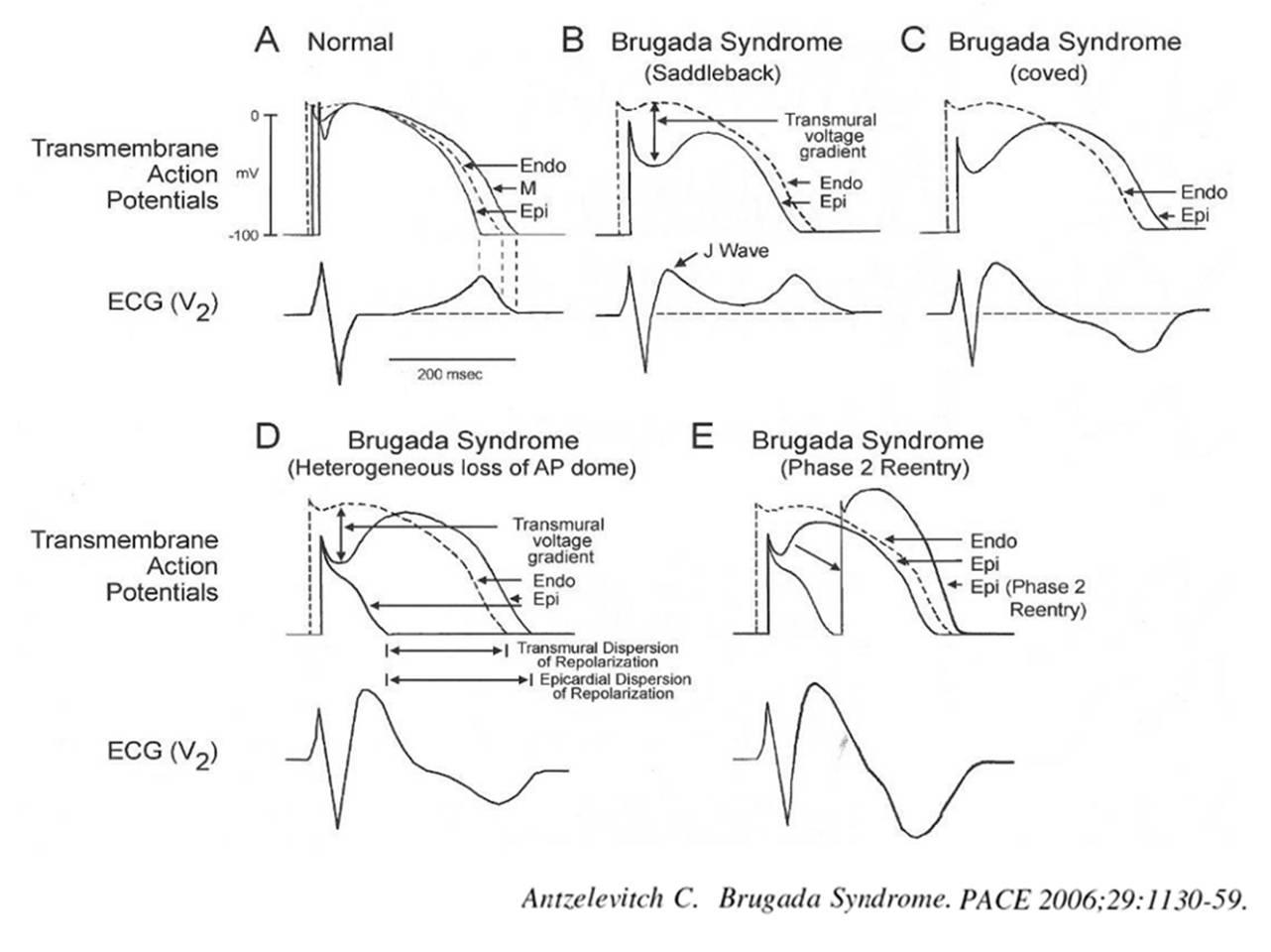
The following slide is a gross summary of the cardiac arrhythmia mechanism

Understanding cardiac arrhythmia is vitally important for a few reasons in a few settings.
- In acute settings, we need to know automatic tachycardias will not respond to shocks. Reentry tachycardias will respond more promptly. (Of course, we may not know it till we shock ) Calcium blockers like verapamil might block triggered activity in MAT. Overdrive pacing is the answer for many automatic tachycardias and some refractory reentrant tachycardias (ATP protocols in ICD has taught us this )
- In the chronic setting when you contemplate mapping, locating, and ablating arrhythmias, mechanisms are important. The task here is locating slow conduction paths and decoding the diastolic circuit around the scar (If you plan ICD, knowledge about mechanism becomes redundant again)
- Finally, knowing the mechanism of arrhythmia is a fascination by itself to help understand the great subject called cardiac electrophysiology, where 100s of ion channels work nonstop drawing the action potential on a moment to moment basis sustaining our life.
A challenge
Can you localize a VT and find the mechanism in a patient who is Ischemic /hypoxic and acidotic? You can never do it. Please note, most polymorphic VTs can’t be localized. The mechanism is either automaticity, trigger activity, or even micro-reentry. You need to shock and look for the causes.(Link to How does the treatment of monomorphic VT differ from Polymorphic VT? )
Final message
Should we need to know about the mechanism of arrhythmia we treat? Definitely yes, if you have that passion to know the truth, or else just order Amiodarone or shock and check out of CCU. (Of course, we have a very good option of calling EP consult the next day.)
A review article on mechannism of cardiac arrhymias
Rev Esp Cardiol. 2012;65(2):174–185