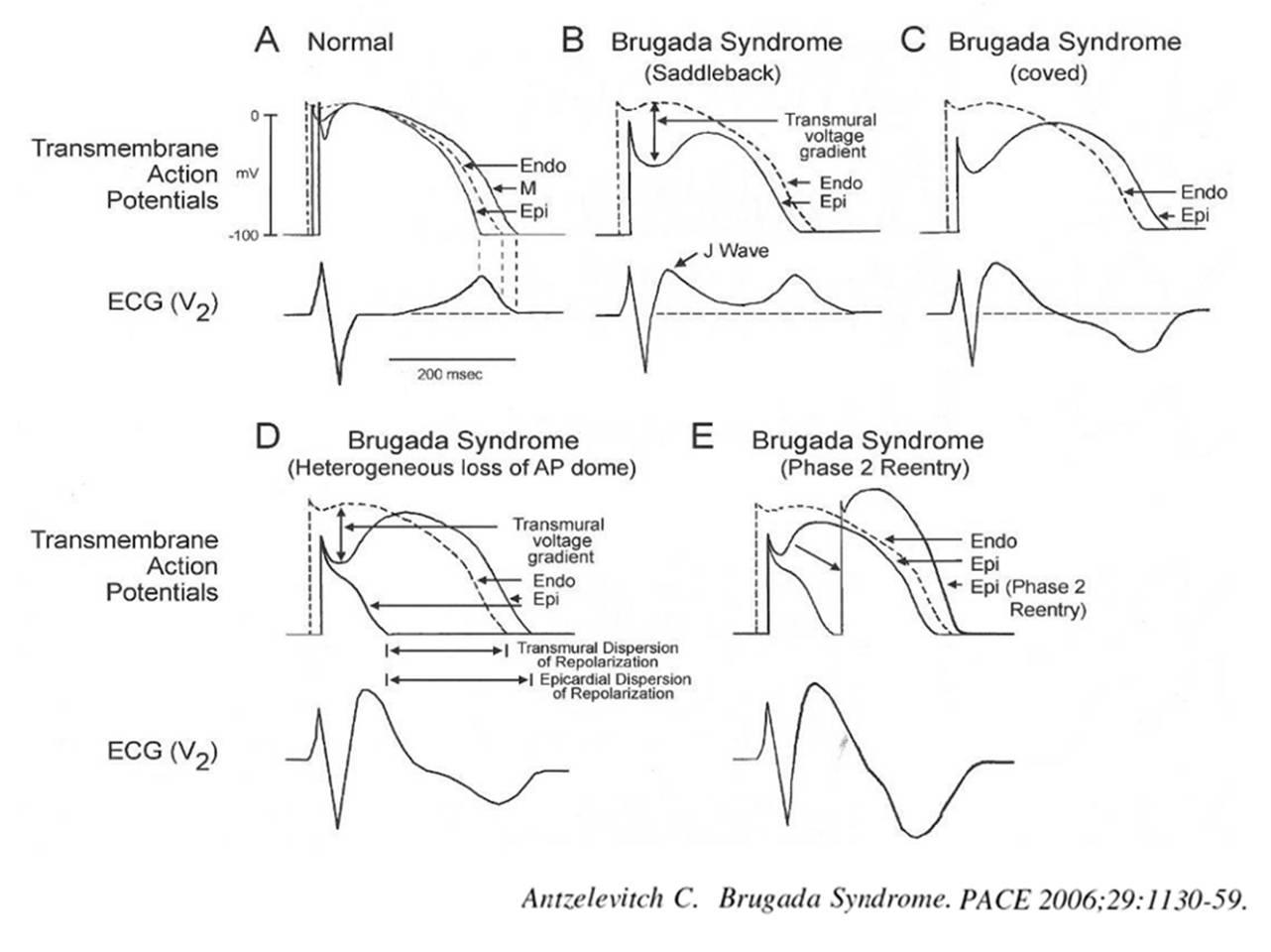
Brugada syndrome is due to a genetically impaired sodium channel activity ( SCN5A) in phase o, of action potential .This results in phase 1 (Ito channel) failing to inscribe the transition between phase 0 and 1 that result in loss of dome .This loss of dome is dominant in epicardial cells compared to endocardial cells.This result in electrical heterogeneity and a hence a voltage gradient in repolarisation phase that can trigger a Phase 2 reentry mediated VT /VF.The above said defects are either dormant, manifest, self extinguishing , dynamic subjected to autonomic tone , ambient myocardial temperature (Febrile VTs) making this a complex entity.
There are three distinct types according to surface ECG.It can be either spontaneous or induced. The arrhythmic events and prognosis and hence management differs according to the types.
 All types carry a minimal risk of SCD , variable though . Of course syncope has to be much more common. Curiously every episode of syncope is seen as naturally aborted SCD by physicians ! (No one to be blamed for this .The definition of syncope is like that !If the patient doesn’t wake from syncope it becomes death !).
All types carry a minimal risk of SCD , variable though . Of course syncope has to be much more common. Curiously every episode of syncope is seen as naturally aborted SCD by physicians ! (No one to be blamed for this .The definition of syncope is like that !If the patient doesn’t wake from syncope it becomes death !).
When a patient with Brugada has a syncope , it doesn’t imply he experienced a dreaded VT or VF.While SCD is invariably due to ventricular fibrillation , a spontaneously terminating VF as a cause for syncope is rare in Brugada . (Ref 2 : ILRs have documented though in few)
So what exactly is the cause for syncope in Brugada ? The issue is real and critical in clinical decision-making. We are beginning to document variety of mechanisms. Following are the possible causes
- Sustained VT or NSVT with
- Non sustained self terminating VF
- Extreme bradycardias (Vaso vagal )
- AV blocks
- Unrelated neurogenic
Final message
It is to be strongly emphasised a significant subset of Brugada patients especially in Type 1 Brugada (spontaneous or drug induced ) the mechanism of syncope is often not related to the dreaded VT/VF. It can simply represent high vagal tone and unexplained dynamism of autonomic activity .ICD is not a default indication for all those with syncope in Brugada syndrome.Think , pause and decide when you deal with such patients. ICDs are true revolutionary devices . . . no two thoughts about it,but it can make a hell out of heaven if used in an inappropriate situation !
Reference



