The ECG changes in ACS can be “as dynamic as” an occluding thrombus. The initial events include sudden total occlusion, early lysis, a trickle of flow, partial re-occlusion, reflow, no-flow, etc. The extent of transmural vs sub-endocardial ischemia, the competing force of re-perfusing vs necrotic wavefront, would define ECG findings. This makes the ST segment labile in the early hours of ACS. This is also the basis of some cases of STEMI evolving into NSTEMI and vice versa.
A 65-year-old man presented to with this ECG,
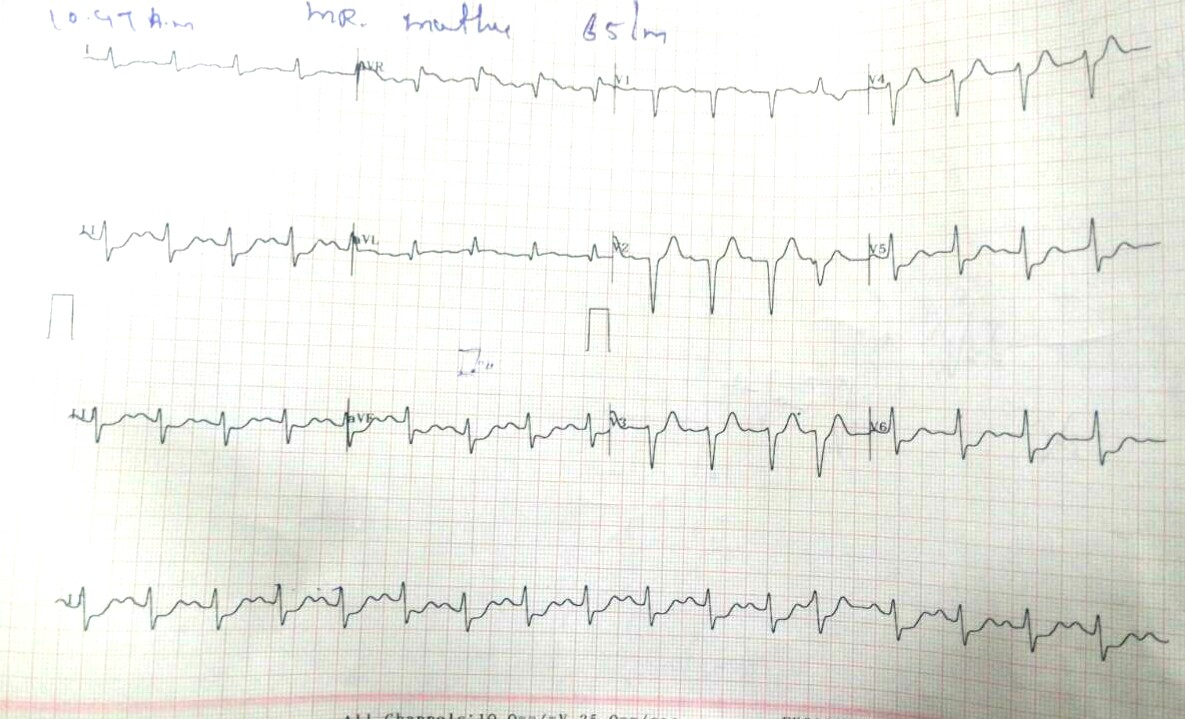
Does this ECG allow you to go ahead for thrombolysis? It actually looks like NSEACS with ST elevation in AVR suggesting left main lesion
The initial diagnosis of NSTEMI was made, and hence thrombolysis was not considered. Even as the fellows were mulling over the diagnosis, one of them could find one more ECG available taken a few hours ago in another hospital.
It had something on it ,
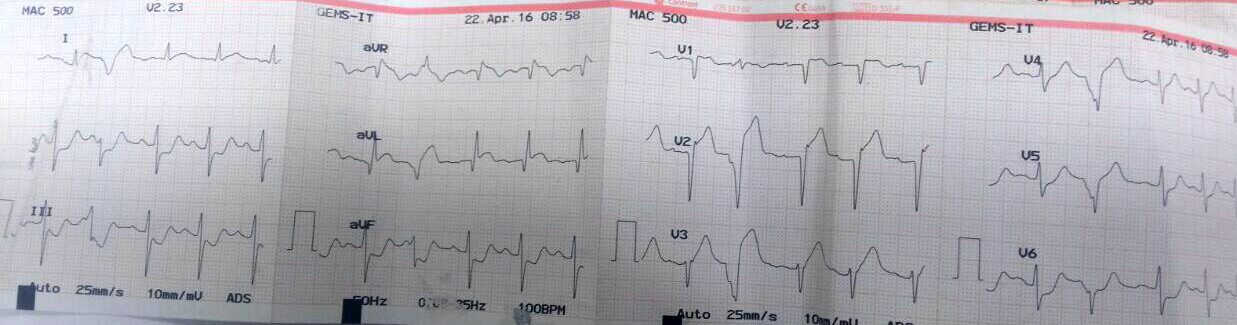
This ECG taken a few hours ago, shows ST elevation in 1 and AVL, and few VPDS in the chest leads unmasks the anterior ST elevation.
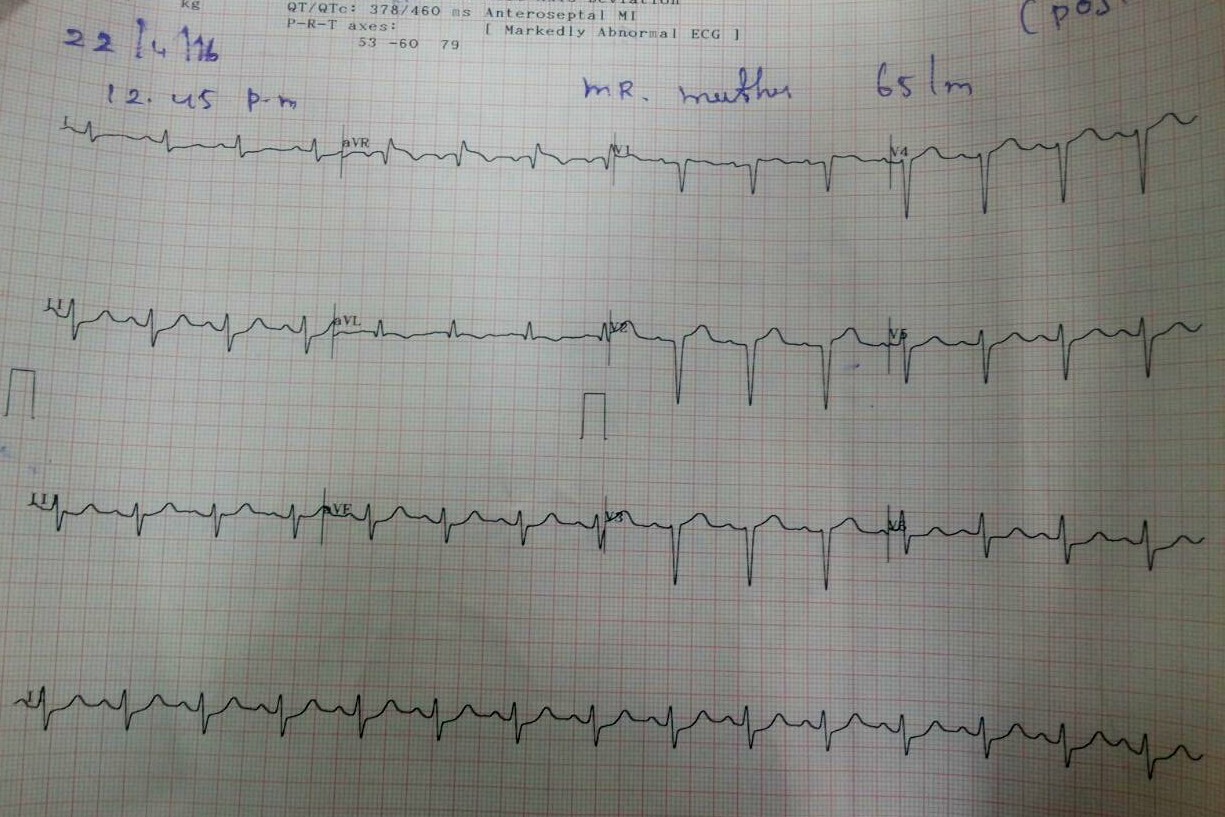
The moment we saw this ECG it was decided to go ahead with thrombolysis.The final ECG after thrombolysis with (Streptokinase) showed further stabilization. The question of thrombolysis in NSTEMI though not indicated in general, in selected situations we need to Introspect!
How to manage a patient who presents as NSTEMI but had STEMI a few hours ago?
Four ways to ponder!
- This patient should not be lysed as we have to treat the current event, not the past. ,(Its NSTEMI and no need for lysis) Just heparin, dual antiplatelets. That will do.
- One can go ahead with lysis as there is evidence for STEMI in prior ECG.
- There is ST elevation in AVR even in the second ECG and so you have to thrombolyse !
- “Come on guys, . . . don’t live in the primitive era of managing ACS in CCU . Forget the ECG take him to the cath lab , suck out all thrombus and deploy a stent and come out”.
* The last one , though appear practical (and most of us would love that ) is an unprofessional way of practicing cardiology. Management of ACS requires sound principles of ECG and its correlation with the Intra-coronary and myocardial pathology.
What happened to this patient?
He did well, free of angina with minimal LV dysfunction. He was discharged. Will be reviewed later, for further evaluation. This is a typical example of a patient with ACS managed successfully without entering the cath lab.(A forbidden practice and a potential coronary blasphemy )
Final message
ECG changes are as dynamic as the Intra-coronary blood flow in ACS. Multiple factors determine ST elevation or depression. While thrombolysis is reserved for STEMI, NSTEMI has little or no benefit to accrue with thrombolysis. However, this is applicable only for de-novo NSTEMI and may not apply for STEMI in transition into NSTEMI as in the above patient.




Leave a comment