With TAVR (Transcutaneous aortic valve replacement ) threatening to take away the Aortic valve surgery atleast in high risk subsets from surgical domain ,a new development is taking place in aortic valve surgery. Minimally Invasive aortic valve replacement and implantation of low profile , bio prosthetic valve placed in aortic root without active suturing .This type of AVR can be done without traditional sternotomy with minimal bypass time , less surgical morbidity and mortality.
It has some specific advantages over TAVR, as the native valve is removed , calcium is debrided and hence less stroke and para-valvular leak .In TAVR cardiologists are blinded ,do lot of guess work to place the valve in right position , struggle to handle the deformed and distorted native valve tissue .My belief is,surgery does a more precision job , since the valve is placed in optimal position .One more issue is, complication of complete heart block and subsequent requirement of pacemaker , its prohibitively high for TAVR as on 2016.(up to 25% )
These new generation valve are expected to narrow the gap between AVR and TAVR. Still. avoiding a surgery is the biggest advantage which drags most patients to TAVR. However, one should ensure quality shouldn’t be compromised for simplicity.
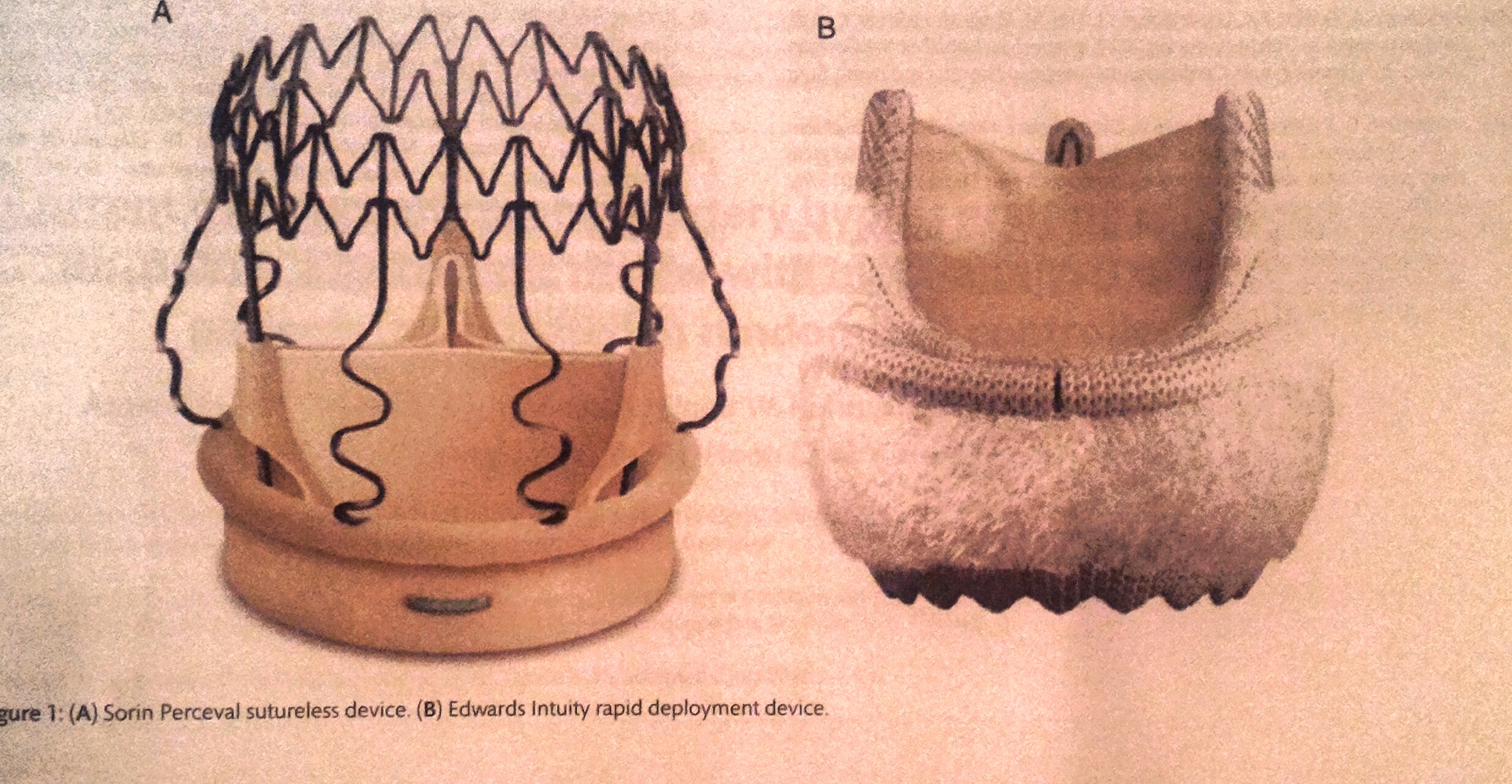
There are two valves available for suture less AVR , both from Bovine pericardium.
1.Perceval (Psorin)
2.Intuity (Edwards)
Evidence
CAVALIER and TRITON (PERSIST -AVR forthcoming)
Message for the patients
TAVR is a revolutionary treatment modality, agreed .However , one need not blindly accept the TAVR if offered especially in low and medium risk* situations just because it avoids a surgery.(*Of-course technology may evolve further ) Discuss with surgeons .Be well informed about all the intricacies.Currently surgical risks seem to overstated and TAVR risks are underplayed in spite of huge cost advantage in favor of surgical AVR.
A note of caution , for suture less AVR must be made .Basically , surgeons tried to imitate the cardiologists, .Ironically , it has the same issues of TAVR for possible migration of valve.Conventional AVR with active permanent fixation sutures will remain the 24 carrot gold standard for AVR and all others may just glitter !
Please realise, medical decision making and consent forms are increasingly looking similar to signing a house mortgage loan which comes with lots of known and unknown “conditions apply”!
Reference





Leave a comment