Significant MR is a contraindication for PTMC. However, If MR jet is central , and mild (some times little more than mild as well ) PTMC can be safely done. The MR may not worsen .It may even disappear.
Note: Eccentric MR jets are indirect evidence for sub valvular disease. Its very likely to get worsened and may require a mitral valve replacement .
Here is patient with severe mitral stenosis, the MR is in all probability safe.
Angle of eccentricity
One must realise , the eccentricity of a jet is not very objective .What may appear as central jet in long axis may be wall hugging in 4 chamber view. This is very important to recognise. Further , even central jets can reveal a invisible eccentricity detected only on 3D MR jet reconstruction.
One simple way to ascertain central jet is to check whether the MR jet align in the same angle as diastolic color jets of MS into LV inflow . (Looking carefully ,the diastolic color jets also provide us info about sub-valvular disease )
More anatomical distortion in this patient
Incidentally , this patient also had another anatomical adversary ie ,the bulge of IAS into right atrium. This can happen two ways .Septal aneurysm or a normal septum bulging to RA due to raised mean LA pressure.
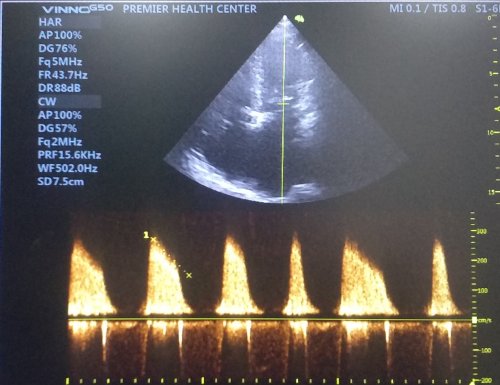
Miral stenosis with Atrial fibrillation showing the changing mitral inflow jet .

The radius of curvature of IAS bulge Indicates its more of septal weakness that contributes than the raised pressure. There is a small risk in these patients the IAS flap may give way during the procedure and a small ASD may be created .(Hemodynamically may not be significant though)
How does the MR disappear after balloon dilatation ?
If you ask this question , it means your are a thinking cardiology fellow , good.
Guess your answer. Its all about physics of MVOs behavior in systole and diastole . The mitral valve tissue attachment and adhesion causes not only a diastolic narrowing but also a fixed systolic regurgitant orifice.Once you relive it the leaflets begins to co-opt normally without a systolic leaky orifice.
Final message
Though there are clear contraindications ,suitability of mitral valve for PTMC is more of a personal experience and confidence. A MR jet of grade 1 may be acceptable. A huge LA, Distorted IAS anatomy, a clot confined to LA appendage are relative contraindication only. The puncture site on IAS , minimal manipulation guide wire within LA, a gentle over the wire technique to cross mitral valve or some of the tips for success.
Never hesitate however to refer complex cases of mitral stenosis to the surgeons. Of course , you can’t insist them to do a valve preserving OMV .It is unfortunate(They have good point of argument as well) most of the surgeons have have made Mitral valve replacement as a default modality
Post ample :
When we were cardiology fellows , we used to have a mitral valve scoring system for suitability for PTMC. Its called Wilkin’s score. Its a purely an anatomical score. (I guess still its expected in Board exams) What we need is comprehensive anatomical and physiological assessment of mitral valve. With due respects to published literature this scoring system lacks two vital parameters we look before PTMC , namely the extent of commissural calcium and degree of MR.



