Cardiologists are grappling with at least half a dozen time windows in the management of STEMI. (It can be combinations of any of the following :Symptom – DAPT Loading – Door – Needle /Balloon-Sheath, wire crossing etc ) Time windows are Important in choosing the right (or no)modality of re-perfusion . Though superiority of primary PCI is thought to be established in academic community , it may not be in real world. Published studies that suggest pPCI is superior to lysis at any time window still lack good evidence.
Why is this long drawn confusion ?
One of the important determinant of outcome in STEMI , is the thrombus organisation (hardening )time . Some how we have assumed PCI can tackle hardened thrombus much better than lysis (In fact the outcome in late PCI is as bad or good as lysis in terms of true myocardial reperfusion in this population.This fact will not be visible in scientific data that’s read superficially .One has to mine deep for the truth) (Claeys MJ,. . Arch Intern Med. 2011;171(6):544–549)
Two more virtual pathological Time windows.
While we are preoccupied with certain time windows in STEMI ,may I suggest two more Invisible pathological windows. I don’t know , whether these are presumptive theoretical stuff , but understanding these time windows will sharpen our decision-making skills in STEMI.
1.Symptom to ATO time (Acute total occlusion)
ery gets occluded(ATO ).This is truly Invisible time window .( Pre-Infarction angina to Infarct time ) Taking the last episode of most Intense pain need not refer to beginning of ATO / Infarct pain. (ACS being as dynamic process in a 24 hour time span an angina can even be post Infarct angina!)
2. ATO to thrombus organising (hardening) time
It is obvious time is primary factor that correlates with thrombus organisation. But there is much more to it. It’s not the fibrin organisation alone that makes a thrombus hard. ATO gets reinforced by plaque and tissue material ( like steel rods inside cement) In other words no one really knows when does the thrombotic process begin or end and hardens thereafter. But we know for certain is tackling a hard thrombus is difficult for both modalities currently we have lysis and PCI*
.(Almost forgot the third modality, yes its humble drug heparin(.It can do wonders little slow though , Slowness doesn’t matter beyond 24 hrs is it not ?) Now there can be a role for Warfarin also to get rid of chronic IRA thrombus (Moon JY, N The role of oral anticoagulant therapy in patients with acute coronary syndrome. Ther Adv Hematol. 2017;8(12):353-366.)
There are excellent studies that correlated time window to thrombus hardness.At least in 50% IRAs with time window less than 12 hrs have thrombus age more than 24 hours Some of the thrombus material aspirated has been shown to be many days old (Kramer et al PLoS One. 2009;4(6):e5817)
Image source : Miranda C.A. Kramer Relationship of Thrombus Healing to Underlying Plaque Morphology in Sudden Coronary Death Volume 55, Issue 2, January 2010
How to arrive at the age of the thrombus ?
It’s a difficult task to guess the age of thrombus with help symptom onset and ECG . There can be 50 % error as discussed earlier.
Is coronary angiogram helpful ?
There is no good clue to differentiate fresh from old thrombus by just looking at angio shot. Some experts are able do it (Guess it ?)
Poke and feel with guidewire : This is probably the best way to tell whether thrombus is fresh or old (Still not fool proof ) Most of us do this in STEMI . All is well if guide wire cuts through smoothly and nice flow is established.(What we call guide wire angioplasty) Procedure is completed with or without a stent ( &residual lesion) .This is the most gratifying and desirable outcome of primary PCI. (Note : Hardness of thrombus can be overcome stiff wires and force.That doesn’t make it a fresh clot ! This is where we may end up with No-reflow)
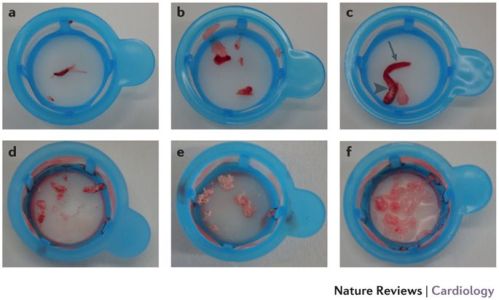
Image courtesy : Karim D. Mahmoud & Felix Zijlstra Nature Reviews Cardiology volume 13, pages 418–428 (2016) Various forms of thrombus aspirated during primary PCI.
When poke test fails . . . be ready for a long haul or quit
Thrombus is not a single aged mass of blood. It has lawyers of clot with different maturity ( like shells over earth ).Hence poking has its own side effects too.Some of it can be violent.When deeper layers of old thrombus is exposed to fresh blood it can create fresh cycle of clot activation.( Ofcourse we fight it out with DAPT and heparin) Winner of this fight can never be predicted. To conquer the thrombus or quit is directly linked to the cardiologist wisdom.
What about OCT/IVUS ?
They could help us to assess the morphology of thrombus and give us Indirect clues about the age of thrombus. Some of the experts say they use it efficiently . My opinion is it adds more glamour than true enlightenment .(Mind you , we need to cross , clear and flush the vessel to complete OCT. The fact that we are able to complete OCT in STEMI settimg would mean thrombus is fresh .In that way it may be useful but without a true purpose.)
Thrombus aspirate analysis : Its more scientific way of arriving at the age of thrombus (Any one want to do carbon dating on this ?) , This again lacks practical use as we need to assess the thrombus age before poking to avoid subsequent complications. It is also not clear whether thrombus in STEMI is more of RBC and fibrin and net platelet content can’t be quantified.This especially true in stuttering ACS where NSTEMI is threatening to become STEMI or vice versa. (Platelets love to hug each other at high shear force , RBCs do the opposite )
Is the Consistency of the thrombus uniform ?
Here comes the importance of the length of the thrombotic segment. It’s estimated the length of the thrombus segment can be anywhere between 1 cm to entire length of the coronary artery distal to the site of occlusion .The initial proximal part may be soft as its directly exposed to DAPT and heparin.The distal thrombus is flushed only with collateral or a trickle of flow from anti-grade .So ,very likely the distal thrombus is harder than proximal.
How does DAPT loading and subsequent heparin interfere with thrombus organisation ?
Loading DAPT has a definite impact and prevents hardening.(But, one issue is it shouldn’t have been happened before administration)
What is the natural history of organised hard thrombus in IRA ?
- It transforms into a CTO.(Many of us believe this is dominant theme)
- Late total recannalisation – 20% by 30 days
- Partial recannalisation (More than 20 % ?)
- Since wide-spread use of predischarge PCI , true natural history is masked.
Final message
Taming STEMI with pPCI is not always a time sensitive emergency procedure . It’s important to recall STEMI patients can harbour thrombus with different maturity .We know STEMI can occur even in patient with chronic thrombotic process also (even a CTO) . This is proven by a simple fact people walk in 3 days after MI casually. Further, during pPCI both early and late arrivals have equal difficulty though they carry different set of problems tackling the IRA.
If we really believe principles of coronary care is aimed at tackling coronary thrombosis , wisdom lies in judicious use of both CCU and Cath lab facilities .Never hesitate to rush back the patient to CCU for a quick lysis (Or Intra coronary) and avoid the potentially prolonged battle against huge mass of hard thrombus.
Reference
Post-ample : A quote
Importance of early arrival of STEMI patient to nearest hospital is huge , not because of the possibility getting an emergent PCI . Rather, it is due to fact that simply reaching the nearest coronary care center dramatically reduce the mortality.(My guess is , this mortality benefit should be more than Lysis/pPCI put together)



