Human physiology can dramatically surprise us.Here is a situation regarding K+ ion and cardiac function.
Low potassium level is a well known cause for skeletal muscle weakness and paralysis.While,in cardiac muscle usually the opposite happens.It is the high potassium levels that depresses and cause paralysis.(That’s why,it is used in cardioplegic solutions. )
But,the classical differences between skeletal and cardiac muscle need not apply in critically low levels of K +
What happens when K + is critically low ?
We know, K + is the vital ion that maintain not only the membrane potential ,(Recall Nernst potential ) but also keeps the action potential floating and dipping with every beat.
Imagine the intracellular chaos when these ion levels changes in dramatic fashion . (Of course,God has ensured very tight regulatory controls at various levels within each cell ! )
However , ECG changes are expected 100 % of time with falling K + especially below 3meq.Surprisingly , low K + levels have little mechanical impact.(Or is it our ignorance,considering the fact , cardiac electrical mechanical activities are tightly coupled?)We have to find answer from patients like this .
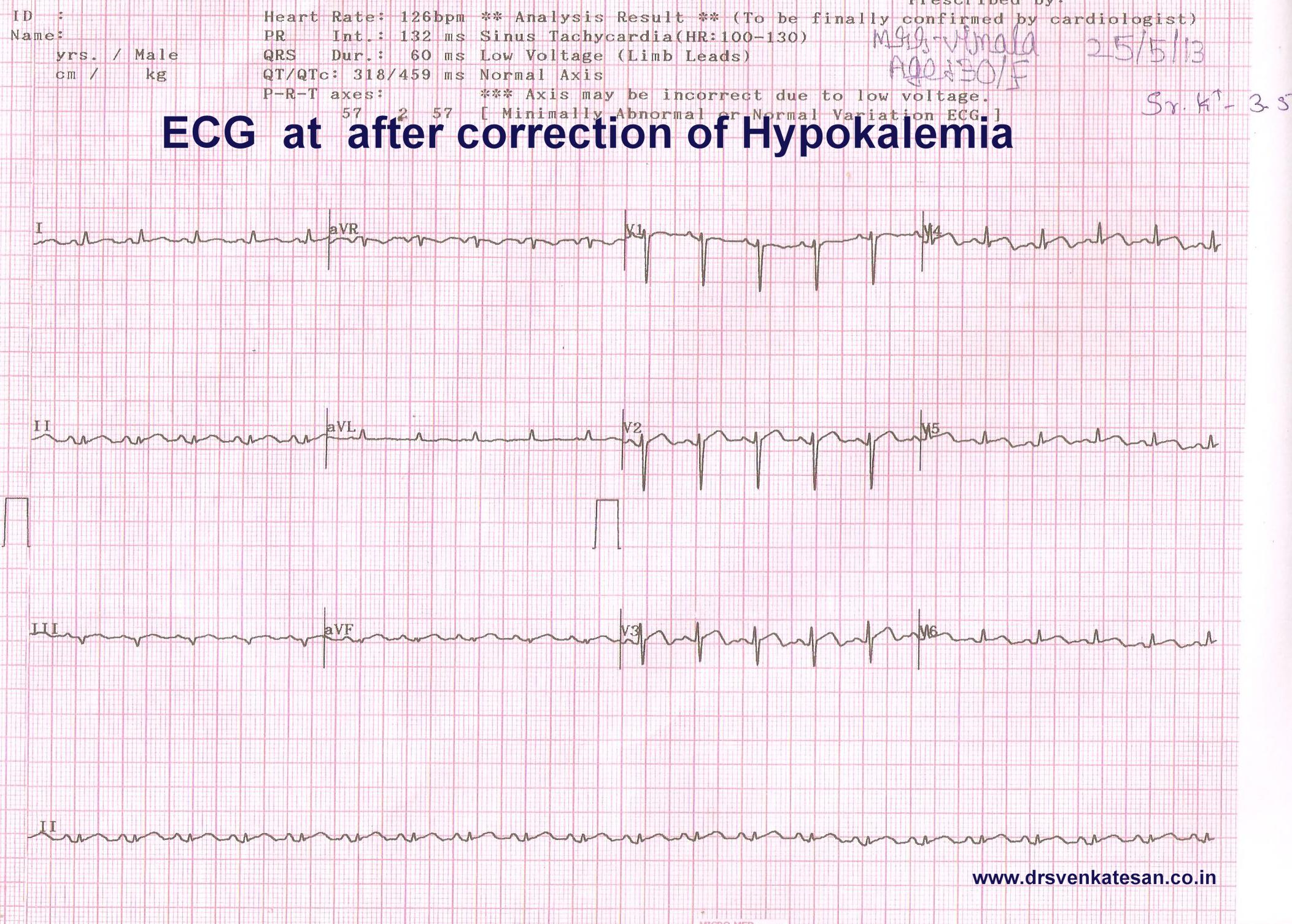
A 30 year old women came with breathlessness and fatigue and her ECG.

Can we afford to miss a diagnosis of STEMI ? With all our collective wisdom STEMI was diagnosed promptly . . . of course wrongly !
She was adviced streptokinase.A shrewd fellow who reviewed the old records spotted the past history hypokalemia , and Inj streptokinase was put on hold.(Lucky patient . . . she was not shifted to cath lab )
Her K + was 2.3 Meq. The LV function was significantly impaired with global hypokinesia, which improved with correction of K+.
She was later referred for nephrology work up , they had made a possible renal tubular disorder for the Hypokalemia.
Clinical Implication.
When potassium levels are critically low myocardial function may deteriorate.Here is a patient with dramatic STEMI like ECG with extreme hypokalemia.
Our ignorance regarding electrolytes and myocardial function remains unexposed .In critical care units wide swinging metabolic and electrolytic parameters are common.ECG is just a marker for these .Similarly all LV dysfunctions are not primary myocardial disorders (Sepsis, Hypoxia, Extreme acidois , Uremia ,drugs,toxin can lead to myocardial dysfunction.)
Experienced physicians do not form hurried opinion.Wait . . . allow things to settle down and assess again.After all ,there is long list of causes for ST elevation other than STEMI !
Reference




I am sure 100% there is something else going on here. This is never a typical ECG for hypokalemia! Hypokalemia is associated with ST depression and not ST elevation.