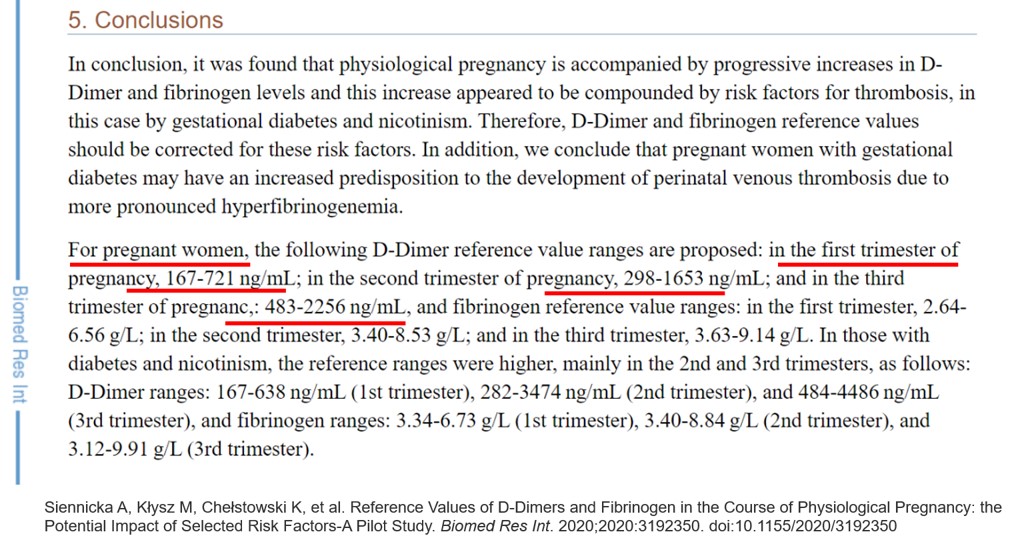
The well known pro-coagulant state of pregnancy is an evolutionary protective process to make blood clot quicker, to save fetal loss in early pregnancy and mitigate postpartum bleeding. Still, in many women, this natural adaptive process confers an enhanced thrombotic risk. The molecular mechanisms for this pro-coagulant state are, there is increased factor VII, fibrinogen, reduced protein S. It is interesting to note, while plasminogen levels are elevated, D-dimer is also increased, indicating an ongoing fight between pro & anticoagulant forces, converting the physiological maternal- placental bed a mini harmless DIC equivalent zone.
There are several important systemic, placental, (Fetal) and cardiac indications for anticoagulants and antiplatelet agents in pregnancy. The list is increasing in a steady fashion. (Most IVF pregnancies seem to need it for some unknown reason)
- Risk of VTE
- Recurrent pregnancy loss(Placental micro-circulation clogging)
- SLE/APLA syndrome /Scleroderma VTE related PAH
- Mitral valve disease with AF. Cardiomyopathy
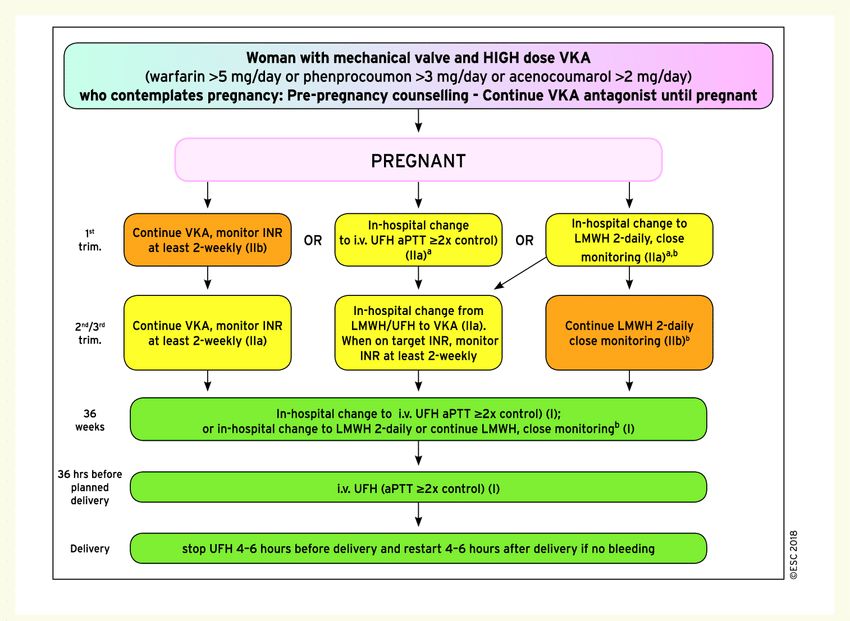
- Finally most importantly prosthetic heart valves & other Intra cardiac devices.
We have few options
- Warfarin (Molecular weight 300 Daltons) is used in dose of 2- 10mg
- Un-fractioned regular Heparin , (40000 Daltons) -Not practical for long term. Used at peripartum phase , just before labor to take control over possible PPH.
- LMWH (Molecular weight 5000 Daltons)
- NOACs are not an option as of now
- Aspirin alone might give partial or near complete protection in some of the above mentioned indication.
General rules
- Warfarin is safe for mother, Heparin is safe for fetus .(both Un-fractioned heparin & LMWH )
- Just because heparin is safe, we cant choose t, it must be equally efficacious too. (Till date no study on LMWH has come to show its efficacy any where closer to Warfarin efficacy, (forget about beating it) in protecting mechanical valve events)
- The concept of bridging till 12 weeks is not mandatory in all
- Switching to regular heparin at term is applicable for both
- Lactation both Warfarin and heparin are safe.(But LMWH is more likely than regulars heparin to appear in breast milk because of low molecular wt. (Ref https://www.medsafe.govt.nz/Medicines/medicine-information.asp)
Is warfarin really unsafe ?
Any anti-coagulant usage in pregnancy is like playing with fire .They have narrow safety window. Further, we must have have a quick antidote in case of dose excess. Warfarin, a powerful VKA, is the time tested key drug despite the well known teratogenic effect. Now we have an alternative LMWH ,which has gained considerable popularity.
The risk of Teratogenicity in warfarin is absolute or is it dose dependent ?
Yes it is dose dependent. (Warfarin causes two phases of side effects one is embryopathy, it also affects later half of pregnancy ie fetopathy with neurological bleeding etc
The Italian connect

Answer to this question came from oldest Romanian city built by the Greeks, Naples, Italy . Dr.Vitale , from the department of Cardiac Surgery, Monaldi Hospital, did this landmark study, way back in 1999 , and convincingly proved , the dreaded embryological side effects are dose dependent. It was done with a meager 58 pregnant women . The conclusions of the study changed the way we used to worry about this drug. It said, warfarin is safe at low doses even in the first trimester , if used <5mg, in terms of embryo and fetal issues. Isn’t it curious that a dreaded drug was made pregnancy friendly by simple study from smart surgeon . It is a real surprise that the conclusion of this study is still can’t be disputed by another big one. Almost all current guidelines use this 25-year-old study to form the core algorithm of current anticoagulant protocol in pregnancy.
Warfarin vs LMWH debate
Teratogen or No-teratogen, coumadin still rules supreme in most high risk situations, especially in women with mechanical valves, (Despite the ease with which this molecule crosses the placental filter , because of low molecular weight -300)
Heparin one of miraculous drug of last century , remains a life saving anticoagulant for various medical conditions. However, its refined version LMWH, though made it more palatable & user friendly, it un-apologetically took the sting out of regular heparin, made it less efficacious (more glamorous though) LMWH usage is in CAD widespread , it has suspect value* in true ongoing ischemia in any active ACS situation. It is strange anti X-a is never monitored in CAD protocol , while in pregnancy we insist on intensive monitoring i. What does it imply ? Monitoring is primarily done to ensure adequacy of anticoagulant activity , rather than risk of bleeding .
In my 30 years I am yet o see a patient have fatal bleed to poorly monitored Enoxaparin. This is the reason the mid trimester LMWH heparin bridge to collapse in many pregnancy anti-coagulant protocols. Now ,we can understand why the veteran VKAs continues to be a flag bearing drug in pregnancy .Of course, INR-guided OAC therapy, though can be tricky, most of us are used to that, unlike the frightful anti X-a troughs and peaks.
*I am sure most Interventional cardiologists will hesitate to disagree with this observation.
2022 update on LMWH : More trouble for LMWH in pregnancy. There considerable concern , that twice a day sub-cutaneous injection may not maintain target anti -X a trough .6-.8U/ml and peak 1 to 1.2 U/ml and currently many centers advice LMWH three times a day ( Bai C, Wu . Medicine (Baltimore). 2022 Dec 30;101(52):e32550.)
Final message
So far, the traditional dictum has been, Warfarin is safe for mother & heparin is safe for fetus. One has to decide accordingly with patient ,spouse & family. I think, its time to tweak this rule, little bit. Warfarin is safe for both mother & fetus* in most patients till 36 weeks in low doses , while LMWH may be more safe , but lags far behind in efficacy, especially in high risk indication. (*Including first trimester but with a lesser proof though)
Postamble
Even in these era of shared decision making, it’s our duty to impress upon our patients (or even enforce) to choose warfarin over LMWH in appropriate times. Don’t simply leave this critical decision to patients.
Reference
Annexure-I (For those who won’t believe this 5mg warfarin narrative, can continue to travel over the turbulent LMWH bridge ) as per the famous UCLA protocol LMWH + Aspirin protocol (From Ref 2)
Further thoughts
I think we need another study ,5, 8 and 10 Warfarin vs LMWH with a prosthetic valve and analyze the fetal bleeding risk in mechanical valves. It may not be a surprise if the cut off of 5mg could move further up.
I don’t know, whether it is a good trend, to note more and more biological vales are implanted at an young age to avoid OAC .These valves have short life span demanding redo surgeries within 10-15 years which may not be not a righteous approach.
(*Mechanical valves can last 25-30 years or more)