Archive for the ‘general medicine’ Category
Sailing the Osler’s ship of medicine in the third millennium
Posted in bio ethics, Cardiology -Patient page, cardiology -Therapeutics, Clinical cardiology, general medicine, Medical education, Medical ethics, medical quotes, Two line sermons in cardiology, tagged clinical acumen, dr venkat quotes, ethics in medicine, evidence based medicine, guidelines protocols, principles of practice of medicine, rcts in medicine, william osler on March 31, 2021|
Syncope evaluation : Clinical cardiology at it’s new low !
Posted in cardaic physiology, Cardiology - Clinical, Cardiology -guidelines, Cardiology -Mechnisms of disease, Cardiology -unresolved questions, Clinical cardiology, general medicine, Syncope, Tutorial in clinical cardiology, tagged clinical cardiology, event monitors in syncope, head up tilt test, holter monitoring, loop recorders, mechanism of syncope, syncope evaluation on December 19, 2013| Leave a Comment »
Recently , I came across a young women who underwent the following three tests for one episode of syncope after witnessing her pet dog bleeding with an Injury !
- Carotid doppler
- Holter monitoring and event monitors
- Brain MRI /MR angiogram
This was followed up by Head up tilt(HUT) in a premier hospital
After 1 week of investigation ,a diagnosis of Neurocardiogenic syncope was made and she was reassured and no drugs were prescribed.
(The collective yield of the above three investigation in fixing a specific diagnosis is less than 10 % of all known causes of syncope )

To diagnose common syncope . . . we need common sense !
Syncope is a dramatic symptom.It is one of the commonest symptom in ER as well . Life time incidence of syncope is at least one episode in 50% all human life ! The definition of syncope until recently , was liberal .Any transient loss of consciousness with spontaneous recovery was termed syncope.
This includes
- Hypoglycemia
- Anemia
- Siezure disorders
- Structural neurogenic (Including , brain tumors , Dural hematomas etc )
- Panic attacks (psychogenic)
Cardiologists wanted to fix syncope as an exclusive disorder of circulatory insufficiency.By bringing in a modification in the definition , ie syncope is now defined as a transient loss of consciousness due to reduction in cerebral perfusion .
This definition helped cardiologists to exclude the above entities . Still many would include all in single basket as patient should be seen as a whole and we can’t expect them to land according to our convenience and classification.
Here is an incomplete* list about causes of syncope (* 99% complete ?)
Vascular
- Vaso- vagal syncope in young ( Neuro-cardiogenic , Common , Benign)
- Autonomic dysfunction of elderly ( Including postural hypotension )
Cardiac
Arrhythmic ( Sinus node dysfunction /CHB/Idiopathic VT/Long QT syndromes)
Structural heart disease
- Valvular heart disease (LVOT/RVOT obstructions)
- Myocardial disease
- Rarely ischemic heart disease
Miscellaneous
- Severe pulmonary hypertension (Including PPH , pulmonary Embolism )
- Paradoxical embolism.
- Aortic arch disease -Takayasu related arteritis .
Investigation
We have a sophisticated array of investigation for syncope .It can be a never ending exercise , ranging from spinal cord evoked potentials to diagnose Shy-drager syndrome , . . . to implanting long-term loop recorders to decode heart beat behavior.
However , evaluation of syncope is the ultimate wake-up call to all current generation cardiologists . . . Why clinical cardiology should never be allowed to die (and it will not ! )
Common sense begins with answering few simple questions . Is it really syncope ?
If you ask this question three times and with specific leads to the patient and the witness , truth will come out . 90% of times it may not be syncope at all (Near syncope, accidental fall, dizziness ,extreme blurred vision, drowsiness etc)
If it is syncope , Is there a non cardiac cause ?
It may related to the Hypoglycemia / Anemia /Panic attacks.Get a neurologist opinion , it would be terrible mistake if you miss a space occupying lesion within the brain. (Missing chronic silent sub dural hematomas is frequent in the evaluation of syncope of elderly !)
Ruling out cardiac syncope is relatively easy
In the remaining patients basic investigation like routine blood tests,ECG, ECHO will help us rule out most serious cardiac disorders.Similarly bulk of the electrical cardiac syncope can be diagnosed.(Holter , carotid study in selected few )
Need for neurologist -cardiologist interaction.
Syncope due to VBI, transient Ischemia attack , Senile vascular dementia is a grey zone . Many have complex neuronal -vascular mechanisms . What is Consciousness ? and What is LOC ? :Is it the lack of blood or severely depressed nerve signal in the reticular activating system? Lots of interaction between cardiologist and neurologist is required to clear our ignorance.(I have one such elderly patient who is intermittently awake ! I call this chronic syncope !) .
Undiagnosed syncope is not a crime
Realise the most important lesson in Medicine . If you have ruled out all serious causes of syncope you should have the courage to be satisfied with that !
Scientific pursuits has a limit. Searching for the mechanism of a psychogenic fainting attacks with intra cerebral electrodes is a clear case of physician acquiring a psychotic behavior !
Final message
Syncope is not only a dramatic symptom for the patient , it also unfolds a drama of costly investigations . . . many with dubious value.
Talk to the patient personally for 10 minutes in a quiet room, try to apply that elusive clinical sense . . . it would rarely let you down !
After thought
What is the true clinical value of * Head up tilt Test (HUT)?
Will be posted soon
When cost of dying . . . exceeds cost of living . . . this world will go nuts !
Posted in Cardiology classics, cardiology-ethics, Cardiology-Statistics, general medicine, Quotes, Social medicine, Venkat quotes, Wintage cardiology, tagged affluent vs poor health care, cost of living, crude detah rate, do not resucitate dnr, ethics in medicine, health budget, health care priorities, health economics, health expenditure gdp, health insurance, health management, health policy for the future, hippocrates, inappropriate health care delivery, mercy killing, obamacare, primary health care, private vs public health care, sharing medical resources, terminal illness, tertiary health care, who world health organisation, withdrawl of life support, world food program wfo on October 29, 2013| Leave a Comment »
News : In any developed nation , 90 % of total health expenditure is exhausted in prolonging final few days of human life !
When cost of dying . . . exceeds cost of living . . . this world will go nuts !
The current real world experience from India’s five star hospitals indicate, many elderly rich men and women spend their last few days before being buried or burnt .They spent an average of 15 lakh Rs per death . This amounts to the entire “life time” cost of living of majority of Indians .
Image courtesy from Flicker/ Rachel sian photostream
When human organ donation is considered a greatest philanthropic act, there is one more excellent alternative for those who can’t do it .If only every super rich translate their cost of dying into cost of others living ! many new lives will bloom .
The exorbitant rise in cost of dying in India , is a recent development and reflects the affluence , honor , pride and of course lots of prejudice lack of wisdom ! Instead of filling the deep pockets of greedy corporates why not the rich add new lives ? !
Final message
Let all elders with irreversible conditions , who have finished their life , shall die peacefully at home .Why don’t we ( Affluent . . . would be cadavers !) cross sponsor their dying cost to a public health , nutrition or medical fund .
After thought
Oh America , . . . Am I right ,? Obama thought it and implementing it too ! I would believe , his health care policy is a small first step in this direction !
Learning crucial cardiology lessons from the patients !
Posted in bio ethics, cardiology-ethics, Clinical cardiology, general medicine, tagged cardiologist cartoon, cardiology cartoons, cardiology consultations, cardiology medical consultations, cartoon medical, clopidogrel, doctor patient relationship, ethics, humour based cardiology, humour in medicine, principles of medicine on July 31, 2013| 1 Comment »
One of my otherwise well behaving patient , suddenly asked me this question , before leaving my clinic after a 15 minute consult .
Doctor . . . I am taking the clopidgrel and aspirin for 5 years like a vitamin tablet . . . is that all right doctor ?
I just got curious, I checked the prescription again . Yeh , he was right !
I have been mechanically writing Tablet Clopitab A since 2008 !

For what ?
Some sort of CAD ! Was it for ACS ? No , it was for chronic stable angina . No PCI, . . . no DES !
Why the hell he is taking dual anti-platelet therapy for 5 years ?
Some body , some where , has prescribed it . This man is taking it for years together with absolute sanctity.
I was amused . . . it is also my mistake . Why it never struck me to scrutinize the prescription ?
I thanked him . I removed clopidogrel from the list , and asked him to continue tablet Ecosprin 150mg for some time .
( And now I had a genuine doubt ! Does he have CAD at all ! I browsed his file , I couldn’t find a true documentation for CAD as I feared !)
I asked him to get back with an exercise test , . . . if it comes negative i can even stop the aspirin as well I explained him ! (Now he got amused !)
Final message
Who wants Knowledge ?
It is dumped every where , free of cost . . . both in real and cyber world .Applying it requires more sense . and my patient taught me that !
Patients not only help us earn our bread and butter , they do enrich our brain as well ! Never get humiliated when a patient teaches you a lesson in medicine !
Why there is so much confusion regarding anti-coagulation following cardio-embolic stroke
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, cerebral circualtion stroke, cerebral circulation stroke, general medicine, tagged acute stroke mangement, aha 2007 stroke guidelines, anti platlet drug in stroke, aspirin clopidogrel in stroke, cardio-embolic stroke, heparin for ischemic stroke, role of heparin in embolic stroke on December 31, 2012| Leave a Comment »
The major issue of contention is fear of conversion of pure ischemic stroke into hemorrhagic stroke .
But here is a catch if you worry about that . . . who will worry about recurrent emboli from heart ?
References
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2678170/pdf/nihms104070.pdf
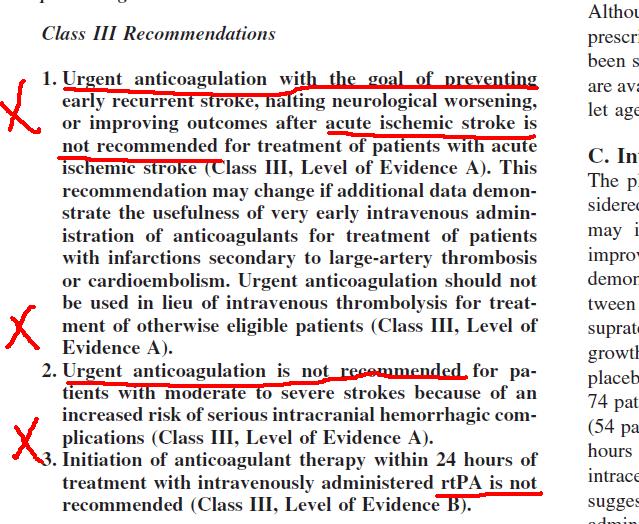
Recommendation for heparin
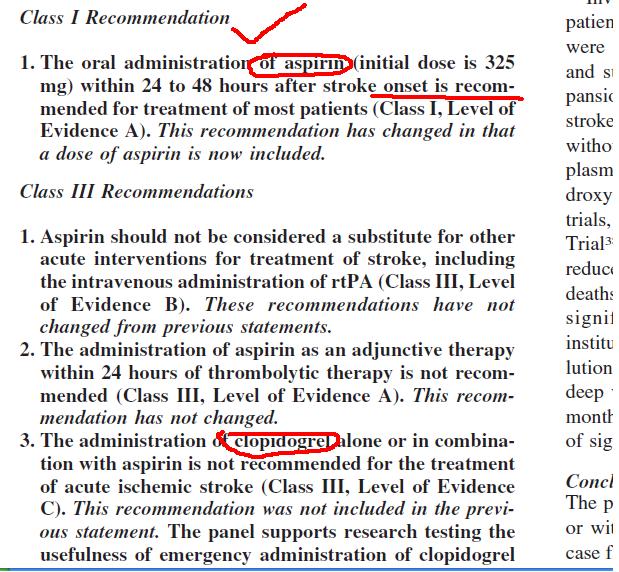
Recommendation for anti-platelet drugs
I think the 2007 stroke guidelines are the latest .Even after going through the guidelines I am not really clear about the answer for the question posed in this article.
One more thing I (mis) understood was , In acute stroke thrombolysis seems to be safe . . . Heparin seems to be dangerous ? Is that true ? It defies logic for me !
One possible explanation is thromolysis is a emergency single shot salvaging process . While prolonged heparin will ooze blood into Infarct ! This is exactly is the reason in tPA should not be followed up with heparin in acute strokes.(unlike STEMI where a follow up heparin is a must )
Regarding prevention of recurrent emboli , we need to bother about whether it is predominately platelet rich or RBC rich
Readers may contribute to find the exact answer !
A comphrehensive review and guidelines for Echocardiogram in Aortic diseases
Posted in Aortic diseases, cardiology -Therapeutics, general medicine, tagged aortic dissection echo, aortic intra mural hematoma, echocardiography of aorta, european assocaition of echocardiography, european society of echocardiography guidelines, tee vs tte for aortic dissection on June 29, 2012| Leave a Comment »
What are the blind spots of aorta in Tans thoracic Echo ?
What are pseudo dissection flops in aortic arch ?
How to differentiate true from false lumen ?
Can TEE also miss any segments of Aorta ?
How is Aortic Intra mural hematoma differentiated form true dissection?
Spend a minimum of 30 minutes in this 14 page article. You will be able to answer all these and much more ! The knowledge gained , would easily beat a day long crash course on Echocardiogram !
Please thank the European society of cardiology for providing this article free of cost !

Reference
http://ehjcimaging.oxfordjournals.org/content/11/8/645.full.pdf+html
Great men in medicine : Virchow is much . . . much greater than his “Lymph node and the Triad” he is known for !
Posted in general medicine, Great websites in cardiology, history of cardiology, tagged father of modern medicine, history of medicine, virchow virchow triad on February 8, 2012| 1 Comment »
Some scientists are known for their discovery , few are known for their vision few for their character .Here was a man who had all of them can be termed as father of modern medicine .

Rudolf Virchow - German pathologist( 1821-1902)
Unfortunately the current generation knows him for his concept and theory of blood clotting or lymph node in the neck .
Here is a reviews about this man who single handedly taught the world
He insisted , caring the sick and treating illness is more of a social science than medical one
We have probably not learnt a single lesson yet , from this master teacher is a different story !


Avid listeners to Virchow in Berlin university
My Virchowian thoughts
This man’s understanding of medicine was much . . . much sharper than us – 100 years ago , when cardiology was practiced with out even an ECG and X-ray chest . ( Is itn’t true today we struggle with loads of 3 dimensinal gadolinium enhanced cardiac MRI ! images )
Virchow’s concepts are most relevant in today’s world , where the corporate and capitalist culture has hijacked the noble profession . Inhabitants of this planet are threatened with eccentrically blown up healthcare system where the development of modern medical modalities is completely out phase of with what is required for the people .
We will pay a heavy penalty if this world continues to witness people die for as flimsy reasons like lack of oral re-hydration fluids , while the other section of society is marketing an exotic mitochondrial DNA slicers for prolonging a cancer victim life by few months .
In a global society where social , economic and environmental responsibilities and liabilities are shared , it would be disastrous if one country is simply not bothered about what is happening in other country.
WHO the world health organization came into being exactly for this reason .
We know . . . how it functions . It is the most abused united nation body . It has neither the required power nor the will to tell the world and insist them the righteous route for human health !
If the rich are not bothered about poor , it is certain the rich will also be eliminated from the planet for the same reasons . . . it’s just a matter of time !
Reference
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1305179/pdf/westjmed00323-0041.pdf
How to become a good cardiologist in 7 minutes !
Posted in dr s venkatesan -Personal, general medicine, tagged best cardiologist india, cardiologist, cardiology fellows training, crash course on cardiology, dr s venkatesan, drsvenkatesan, ethical cardiologist, good cardiologist, madras medical college, teaching video in cardiology, venkatesan sangareddi on August 18, 2011| 11 Comments »
Why doctors are referred to as “Practicing” Medicine
Posted in bio ethics, cardiology-ethics, general medicine, Uncategorized, tagged art of practice of medcine, bio ethics, doctor patient relationship, ethics in cardiology, ethics in medicine, experimental medicine, hippocrates, medcial ethics, modern medicine, patient vs physician, principle of practice of medicine, why medicine is not science on August 1, 2010| Leave a Comment »
It is often quoted “Practice makes every one perfect” . . . Doctors continue to practice for ever . . .If practice is only a rehearsal , when do they perform for real ?
And , we know a doctor spends his entire life time practicing . . . In other words doctors are only experimenting .
So , do not get fooled by his errors . Errors are bound to happen during their practicing sessions !
 The problem with general public is , they never understand this basic fact – medical science is nothing but a , on going research on human body .If only we understand this we can accept the millions of medical mistakes* that occur every day in the global medical profession . The major aim of modern medical science is to reduce that .
The problem with general public is , they never understand this basic fact – medical science is nothing but a , on going research on human body .If only we understand this we can accept the millions of medical mistakes* that occur every day in the global medical profession . The major aim of modern medical science is to reduce that .
* Of course, negligence is a punishable offense . But, we should also realise , non- negligent medical mistakes are many fold higher than negligent ones .
While a careful doctor will avoid negligent mistakes a thinking doctor will avoid non -negligent mistakes also.
This puts onus back on doctors. We need to critically analyse , every
treatment modality we follow .

If you are a strong believer of “Medicine is indeed a science and doctors are scientists ” , please read this article from British medical journal and conclude yourself.

http://www.bmj.com/cgi/content/full/328/7454/0-h
Further reading
The bestseller How doctors think
Picture courtesy : Jupeter stock Images
What is isolated diastolic hypertension ?
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, Cardiology hypertension, general medicine, Infrequently asked questions in cardiology (iFAQs), My presentations, tagged allhat, amlogard, anti hypertensive drugs, hypertension, hypertension clinic, ish, isolated diastolic hypertension, isolated systolic hypertension, jnc, kaplan, mean areterial pressure, sweeny on February 8, 2009| Leave a Comment »

- Hypertension is major determinant of cardiovascular health of our global population
- Millions suffer, hundreds of societies , and as many guidelines , and drugs are still struggling to control the menace.
- An important sub group of HT , (ie IDH ) population has been neglected and never received the scientific interest , which it deserves !
- In our study it occured in 7.2% of all HT patients.
- JNC, the world authority on HT never considered IDH as a separate entity, and as of now there is no specific guidelines.
- And the irony is complete . There is not a major study available to analyse the differential effects of anti hypertensive drugs on systolic and diastolic blood pressure.
If a patient with the BP of 120/96 asks you , “Doctor , will the drug, you have prescribed , selectively lower my diastolic blood pressure ” what will be your answer ?
A clear , I don”t know !
The following paper was presented in the World congress of cardiology Sydney 2002
Isolated Diastolic Hypertension
S.Venkatesan,S.D.Jayaraj.Gnanavelu, Madras Medical College. Madras, India.
Abstract : Systemic hypertension continues to be a major determinant of cardiovascular morbidity. While isolated systolic hypertension(ISH) has been identified as a specific clinical entity, isolated diastolic hypertension(IDH) has not been reported as a separate group. When we analysed our data from our hypertension clinic we found a distinct subgroup of patients who had elevated diastolic blood pressure with normal systolic pressure. We report the clinical profile of these patients. 440 newly registered hypertensive patients between the year 1998-99 formed the study population. All patients with secondary hypertension were excluded.. IDH was defined as diastolic BP more than 90mmhg and systolic BP less than 140mmhg.
IDH was present in 32(7.2%) patients. The male female ratio was 3:1, mean age was 42(Range32-56) The mean diastolic pressure was 96 mm (Range 90-110).The mean systolic pressure was 136mm(Range 128-140). LVH was observed in 4 patients(12.5%). Diastolic dysfunction was detected by echocardiography in 20patients.(62%)
We conclude that isolated diastolic hypertension constitute a significant subset among hypertensive patients and they need further study regarding the pathogenesis, clinical presentation and therapeutic implication.
Link to PPT will be available soon .
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- August 2026 (1)
- July 2026 (6)
- June 2026 (9)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,713,332 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

