Syncope is one of the common, yet difficult symptoms to evaluate especially in the elderly. Post-prandial syncope is one condition likely to be missed out.As the name suggests It has a distinct relationship with food intake. Mild fall in postprandial BP is an expected response but if it exceeds a limit* syncope is triggered. (*Highly variable)
Hemodynamics of Postprandial state
- Normally splanchnic circulation demands up to a 25% increase in blood volume after a moderately large meal.
- When this happens there must be compensatory vasoconstriction elsewhere especially in muscles. Lack of this response results in inappropriate falls in SVR. (The second mechanism is more constant and can be disproportionate to fall of BP)
- The mediators for this are either neurogenic or hormonal or both.
- Gastrointestinal mediator (Vasoactive Intestinal polypeptide dysregulation) is thought to play a major role.
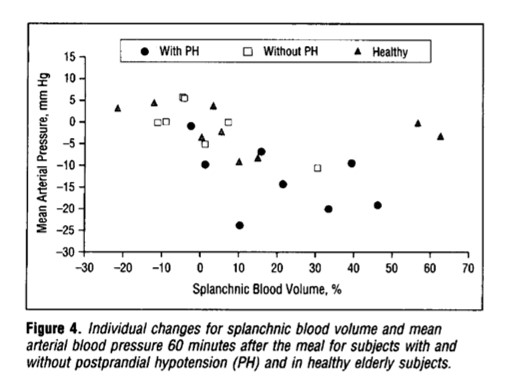
From Jansen et al Archives of Internal medicine 1995
When does it occur?
It can manifest as early as 15 minutes, up to 2 hrs. The fall in systolic BP is around 20mmhg. More common with large, hot meals. The fact that it can occur up to 2 hrs post meals, there is a likelyhood we might overlook it in history.
Other differential diagnoses
- Has a very close two-way link with diabetic patients.(Neuropathic & metabolic ) Postprandial Hypoglycemia-related syncope must be ruled out. (A review)
- Gastrointestinal issues like gastric tumors associated with or without MEN syndrome and insulinoma etc.(Prídavková D, World J Clin Cases. 2020 )
- Two other entities Orthostatic hypotension of the elderly and POTS syndrome are close associates of this condition.
Management
There is no specific therapy. Some of the following might be effective.
- Caffeine,
- Somatostatin,
- Acarbose,( α-Glucosidase Inhibitor )
- Avoiding acute high carbohydrate intake.
- A psychogenic component can be noted in a few that is attenuated by cognitive-behavioral therapy.
- Midoridine, an Alpha¹ receptor stimulant can be surprisingly more effective in some who have overlap with orthostatic hypo (Cleve Clin J Med. 2010 May; 77(5): 298–306.)
Final message
Postprandial hypotension/syncope is a less recognized entity. As always, history is the most important diagnostic tool in the evaluation of syncope, which comes free of cost as well. The diagnostic yield is much greater than sophisticated Holter and event monitors.
Please note, there is a much more prevalent, lesser version of this condition, ie postprandial dizziness or giddiness. However, as already stated there is a significant overlap between orthostatic hypotension and postprandial syncope. It’s worth ruling out diabetes and autonomic dysfunction, (even subclinical Parkinsons) in elders with such symptoms.
Reference
Here is a comprehensive and elegant study (I think, It is only one of that kind on this topic )
Postprandial hypotension Jansen1995






