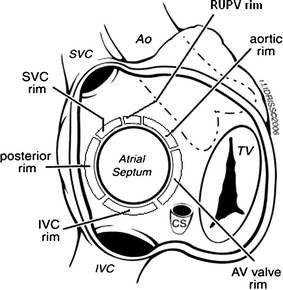
The inferior vena cava (IVC) rim is the most critical rim for successful transcatheter ASD device closure due to its role in preventing device embolization and prolapse. Absence or deficiency of the IVC rim is often a contraindication, as it leads to higher rates of procedural failure compared to other rims like the aortic or SVC.
Anatomical Reasons
The IVC rim forms the posteroinferior border of the secundum ASD, measured in the bicaval TEE view as the distance from the defect’s inferior margin to the IVC ostium. Without ≥5 mm of adequate IVC rim, the device’s right atrial disc lacks stable septal anchorage inferiorly, allowing slippage toward the compliant, funnel-shaped IVC-RA junction. This contrasts with superior rims (SVC), where the SVC-RA junction provides firm foundation.
A dislodged device Video source : APCIS 2016 Jae Young Choi (Yonsei University, Korea)
Physical and hemodynamic forces at IVC:RA junction
High-volume IVC blood flow (2-3 L/min, 60-70% of venous return) directly strikes the inferior septum and device, exerting continuous shear force that can dislodge a poorly anchored disc, causing left disc prolapse into the RA or embolization. SVC flow (1 L/min) is less voluminous and angled favorably, reducing its destabilizing effect.
If there is good rims on all other sides (270 degreees) can we proceed with ASD device ?
Some cardiologst believe so. Some institutions have reported ASD device closure in deficnet IVC rims as well . This is not respecting the evidence (Ref 4,5) But, the fact seems to be different. The IVC’s perpendicular, high-momentum jet amplifies dislodgement. Even good superior/anterior rims fail to counter this inferior “pull,” as the device tends to tilt around the waist, under the dyanmic atrial pressures and flow. Hence IVC deficiency predisposes to instability despite the availablity of 270° of other rims.
One caution : A common mistake done is eustachian valves is taken as false IVC rim and the device is implanted and later facing issuers. So, a meticulous TEE imaging is neccessary .
Reference
- Amin Z. Considerations for ASD closure. Cardiac Interventions Today. 2014;7(2):1–8.
Link: https://citoday.com/articles/2014-mar-apr/considerations-for-asd-closure - Amedro P, Bayburt S, Assaidi A, Kreitmann B, Habib G, Fouilloux V, Fraisse A. Should transcatheter closure of atrial septal defects with inferior-posterior deficient rim still be attempted? J Thorac Dis. 2019 Mar;11(3):708-716. doi: 10.21037/jtd.2019.02.89. PMID: 31019758; PMCID: PMC6462671.
- Song J. Comprehensive understanding of atrial septal defects by imaging studies for successful transcatheter closure. Korean J Pediatr. 2014 Jul;57(7):297-303. doi: 10.3345/kjp.2014.57.7.297. Epub 2014 Jul 23. PMID: 25114689; PMCID: PMC4127391.
- Remadevi KS, Francis E, Kumar RK. Catheter closure of atrial septal defects with deficient inferior vena cava rim under transesophageal echo guidance. Catheter Cardiovasc Interv. 2009 Jan 1;73(1):90-6. doi: 10.1002/ccd.21756. PMID: 19089959.
Postamble
Can we create a neo IVC rim by some means?, (Ex by agumenting the lower end of the IVC with stent , that can protrude clost ASD and act as a rim . We have strated closing the complex sinus venosus ASD, so , this might also be possible)