The 12-lead ECG is the single most important investigation that has withstood the test of time for over 100 years. I think it will never lose its relevance in cardiology. However, the traditional sequence of the 12 lead printout could have been a little more user-friendly, especially in its ability to convey the anatomical orientation. Expecting some Innovation in the ECG reporting format.
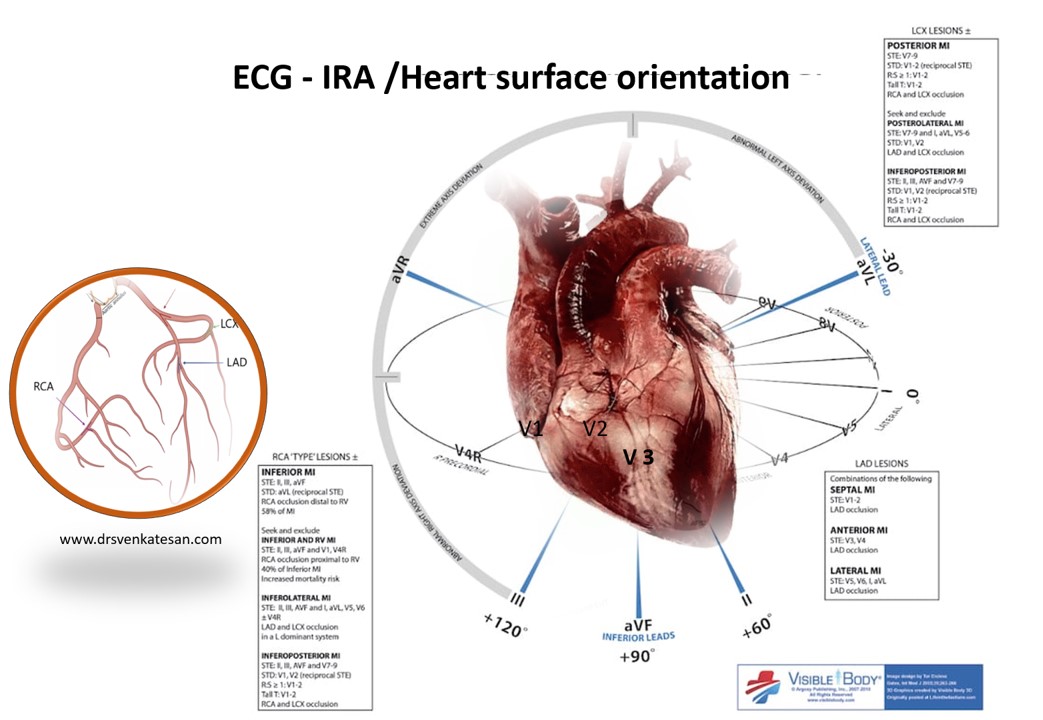
This illustration helps us to understand, ECG lead orientation, and coronary arterial territory, IRA localization with reference to the various surfaces of the heart. (Courtesy of visible body-modified ) Always remember the heart is an organ, made up by a complex fusion and rolling of bundles of muscles over a fibrous skeleton. It has multiple surfaces. Please avoid calling various surfaces of the heart as walls (Request the young medical students to un-tune their brain, from the inherent tendency to Imagine the heart as a well-demarcated four-chambered concrete structure built with bricks !)
Animated version
Currently, IRA localization with ECG may seem to be a redundant exercise, as we are straightaway seeing the coronaries if taken for primary PCI or at least within 24-48 hrs mostly.
- But, IRA localization gives us a rough idea(still useful) of what we are going to deal with during the PCI.
- More importantly, multivessel CAD during STEMI can be very significant in the elderly, diabetic, and in women, which can sometimes confuse us about the real culprit artery. (Recanalised IRA vs other chronic lesions). Similarly, CTOs can masquerade as ATO and vice versa. Here, ECG will come in handy to identify the true culprit.
One useful tip in IRA localization of LAD
Lesions proximal to D1 will depress the ST segment in inferior leads. In other words, if reciprocal ST depression is seen in inferior leads it is most likely a proximal LAD lesion. Paradoxically, in distal LAD lesions, ST elevation occurs in 2,3,AVF. (What may look like a global MI, is in-fact less sinister since it is a distal LAD Infarct)
* The wrap-around LAD* can also mimic distal LAD lesion with simultaneous Inferior and anterior ST elevation. *The wrapping needs to be complete and reach almost the crux (Super dominant LAD ) to cause ST elevation in 2,3, AVF.
Final message
The limitation of surface ECG in localization is real
- Multiple IRAs or diffuse lesions, and collaterals all can confound the ECG -IRA correlation.
- There can be overlap between large diagonal, Ramus (or even a large OM) when they all try to converge on the curvey and imaginary slope between the anterior lateral wall
- Localization of IRA (Rather Angina-related artery (ARA) is a different exercise altogether.
- Experienced operators will agree there have been many occasions, where multiple diffuse lessons with delicate collaterals interwoven make IRA identification so difficult, and ultimately primary PCI is abandoned, and the patient returned back into CCU for lysis (Fortunately, Tenekteplace, and streptokinase never need to bother about IRA localisation you know !)
Reference
A useful review on this topic
Rafl an S, Kamal A. Localization of the occluded vessel in acute myocardial infarction. J Cardiol Cardiovasc Med.
2020; 5: 029-033



