LV dysfunction is one of the most commonly used terminology by cardiac professionals.It can be systolic, diastolic or global, regional etc. But, before dysfunction sets in, the heart fights. The Left ventricle can behave in many different ways when confronted with stress. It increases the force of contraction, elevates it’s Intra cavitary filling pressure and still accomplishes its task of pumping adequately. Further, It can build fresh muscle (LVH). It can double up with more heartbeats. (All these factors are referred to as cardiac reserve mechanisms)
These reserve mechanisms can be activated in the short or long term. In the long term, autonomic activation with neuroendocrine factors joins the compensation process. These will work for some time till the circulatory system settles down to new homeostasis. However, they become counterproductive and becomes decompensated, ultimately heart failure sets in(Unless Intervened)
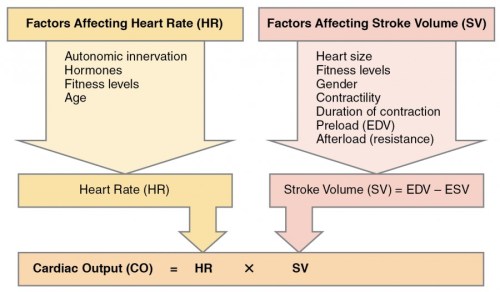
Mechanisms of cardiac reserve. Image source: https://courses.lumenlearning.com/suny-ap2/chapter/cardiac-physiology/
Is LV dilatation a mechanism of cardiac reserve ?
No one calls LV dilatation as a reserve or compensatory mechanism. (I wonder, why not ?) I think like RV , LV too has some potential to reversibly dilate . The quantum of which we are unable to estimate.This happens usually in response to chronic volume stress* like regurgitant valves or high output states. Though cardiomegaly and a huge heart convey a sinister outcome, many hearts shrink if the primary issue is corrected.(Typically in Anemia, Beri Berri. We also know LV may transiently dilate in response to some toxic /pregnancy-related cardiomyopathy.
* Mind you LV poorly tolerates acute volume stress as in Acute AR/MR
The critical gap in our understanding is about this question.
When does LV dilate physiologically and when pathological persistent LV dilation sets in (The absolute state of irreversibly lost cardiac elasticity.) We also know dilated LV will consume more oxygen due to enhanced wall stress (Laplace law) and hence its possible LV dilatation begets further dilatation. Optimal timing of mitral and aortic valve replacement in patients with AR and MR directly depend on this knowledge.
Final message
We need clarity in the following queries
- Is LV dilatation (with normal EF ) a sign of LV dysfunction?
- If so at what level of dilatation?
- Since LV dilatation occurs in diastole can we fit this entity “Isolated LV dilatation” in the already confused spectrum of diastolic dysfunction?
Let us wait for the knowledge to evolve. Young cardiologists could take up this area for research.




