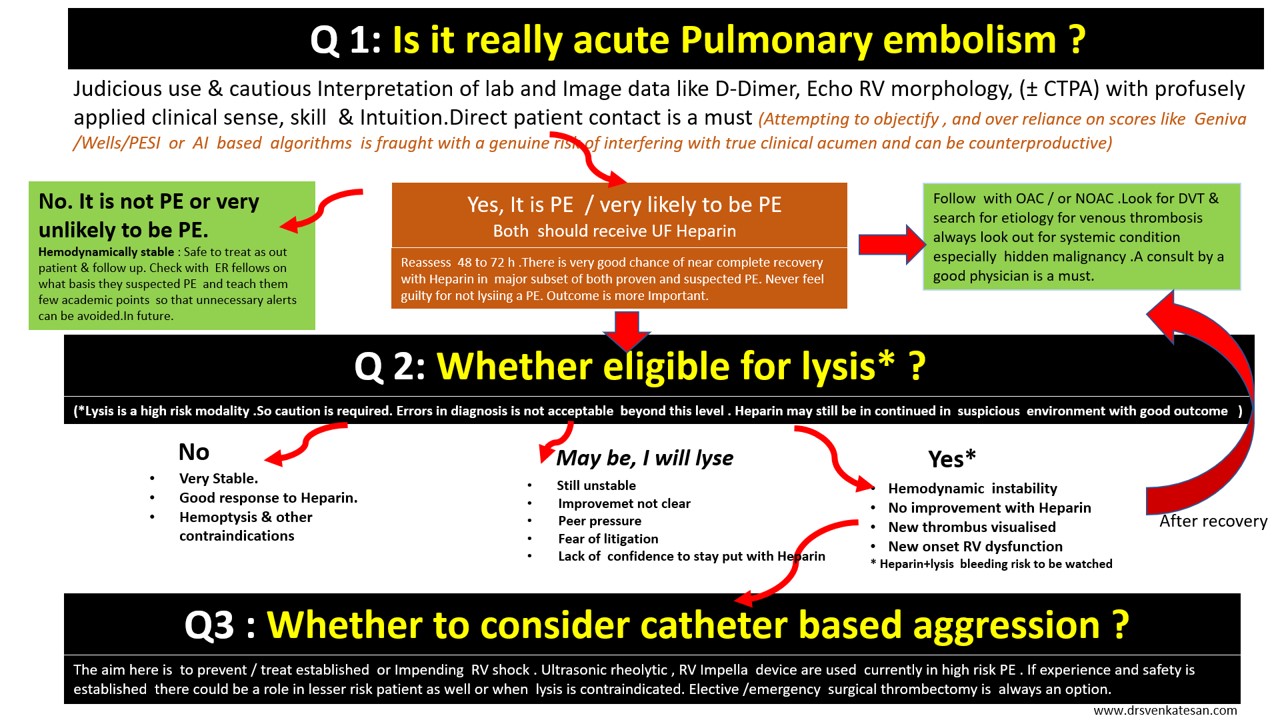
Here is a 3-minute algorithm for the management of acute pulmonary embolism. Just need to ask 3 questions.
Caution: User discretion is advised. Tainted with reasonably acceptable levels of non-scientific content.
Click over the image for a high-resolution slide
Some more critical questions need to be answered.
What is hemodynamic stability?
It is purely based on clinical signs and judgment.(One need to be doubly sure to rule out hypovolemia and sepsis-related hypotension)
Is RV dysfunction equivalent to hemodynamic stability?
No, it is not. Clinical instability must be associated.( The dogma is, if the patient is stable even if there is significant RV dysfunction by echo , that RV dysfunction is not attributable to the current episode of PE)
Can we diagnose and proceed with lysis without CT pulmonary angiogram confirmation?
Yes, you can, provided your suspicion is too strong or you have the extraordinary talent to argue/defend even a fatal bleed ( with your boss or in medical audit ) in a patient who was subsequently proven not to suffer from PE .
How to switch over to Lysis from Heparin alone protocol?
Occasionally one may require to do it. There is an added risk of bleeding here. It can’t be avoided in some situations as Initially, it appear as low-risk PE later on becoming more Intense. Generally, high-risk unstable patients should receive lysis straightaway.
Is 60/60 sign is really useful in deciding lysis?
60 /60 sign tell us if Pulmonary artery acceleration time (PAT) and the TR jet both are less than 60 the likely hood of PE is high in a patient with suspected PE.
- This sign recently got popular not because of its utility, rather because of its simplicity and attractive caption.
- It may be very specific but least sensitive (<20%) So it can never be used as a screening test.
- It also fails to differentiate chronic RV dysfunction from acute RV dysfunction.
- The PAT is strongly influenced by RV dysfunction (It pulls it down below 60 as PAT is dependent on RV Dp/Dt and falsely diagnosing PE
- 60/60 sign adds up to the value of Mconllels sign and can confirm PE with almost 100% specificity.



