Answer is question is wrong : RAA clot do occur in AF and severe right heart failure.It is less often recognised , since echo views are difficult and clinical events are silent.
 Brief account of RAA clot formation
Brief account of RAA clot formation
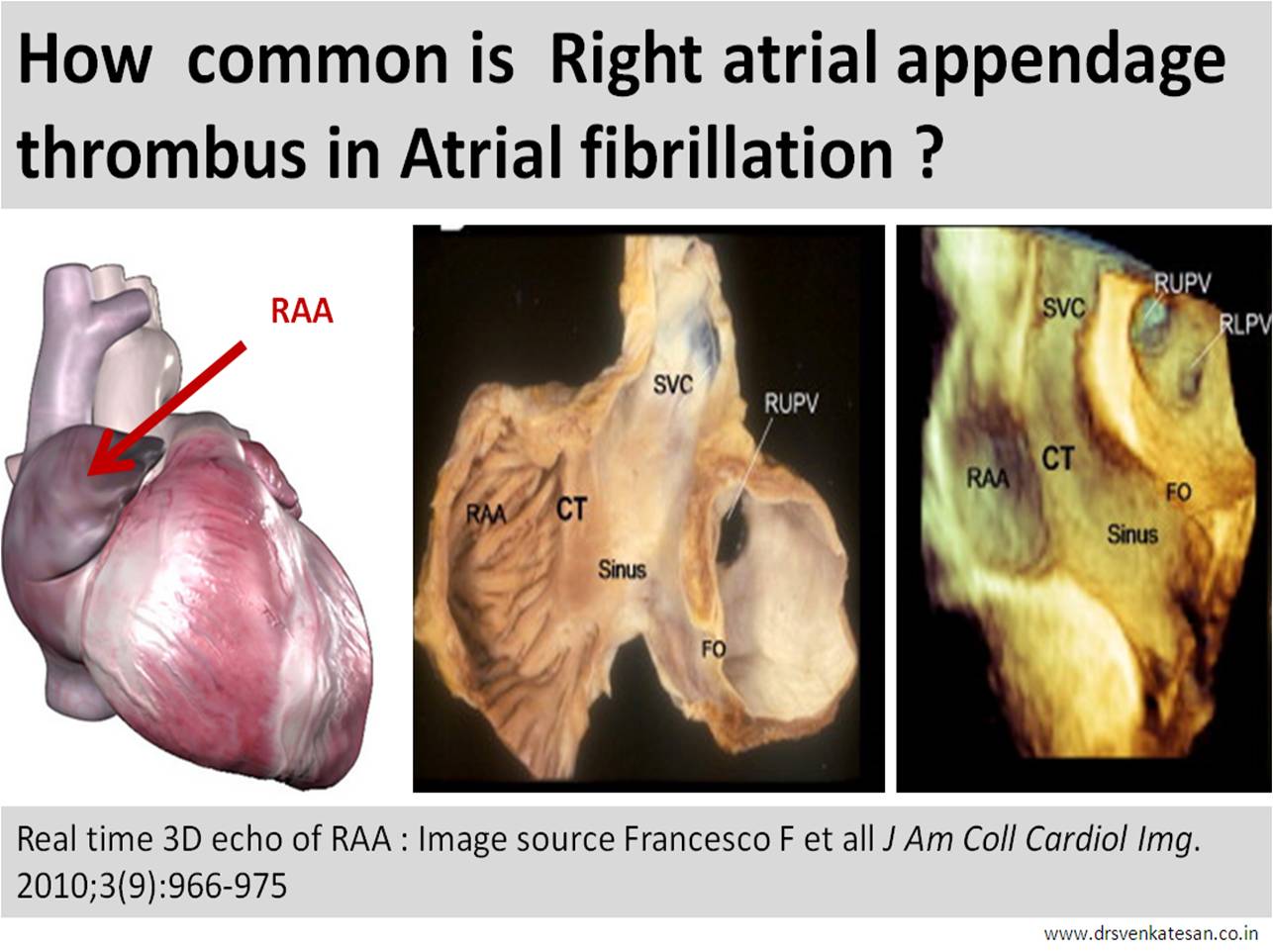
- RAA is broad flat ,thin , chamber comparable to elephant’s ear.The ostium is not that distinct as the body as it blends with crista terminalis .
- Rough pectinate muscles should make it prone for thrombus.Further , RAA has more sluggish flow than LAA increasing the propensity for thrombus.However , the flat nature of the chamber , absence of tortuous tracts , constant SVC flow which is abutting the RAA can counteract this.
- RAA clots are less recognised as echo views are difficult .TEE is often required.
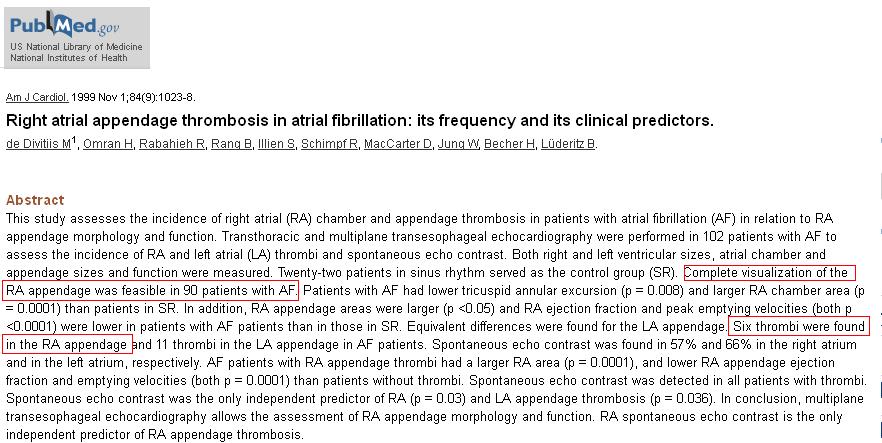
- Overall RAA clot is 50% less common than LAA.
- RAA clot should be specifically looked for in chronic AF and any severe right heart failure. (Unlike MR jet TR jet has less efficiency in flushing the Right atrium )
- Finally,clinical events from RAA clot are less conspicuous as the emboli reaches the pulmonary bed silently.Unlike its colleague on the left side it neither triggers TIA nor a stroke !
Reference
1. Buğan B, Baysan O, Demirkol S, Güngör M, Yokuşoğlu M. Right atrial appendage thrombus in a heart failure patient with sinus rhythm. Gulhane Med J. 2011; 53(3): 214-215.
2.Subramaniam B, Riley MF, Panzica PJ, Manning WJ. Transesophageal echocardiographic assessment of right atrial appendage anatomy and function: comparison with the left atrial appendage and implications for local thrombus formation. J Am Soc Echocardiogr.; 2006; 19(4):429-33.
3.Sahin T, Ural D, Kilic T, Bildirici U, Kozdag G, Agacdiken A, Ural E. Right atrial appendage function in different etiologies of permanent atrial fibrillation: a transesophageal echocardiography and tissue Doppler imaging study. Echocardiography;2010; 27(4):384-93
4 .Ozer O, Sari I, Davutoglu V. Right atrial appendage: forgotten part of the heart in atrial fibrillation. Clin Appl Thromb Hemost; 2010; 16(2): 218-20