This is the Image of JVP wave forms from the famous original paper by BORST JG, MOLHUYSEN JA. in 1954 paper in Lancet.(Ref 1)
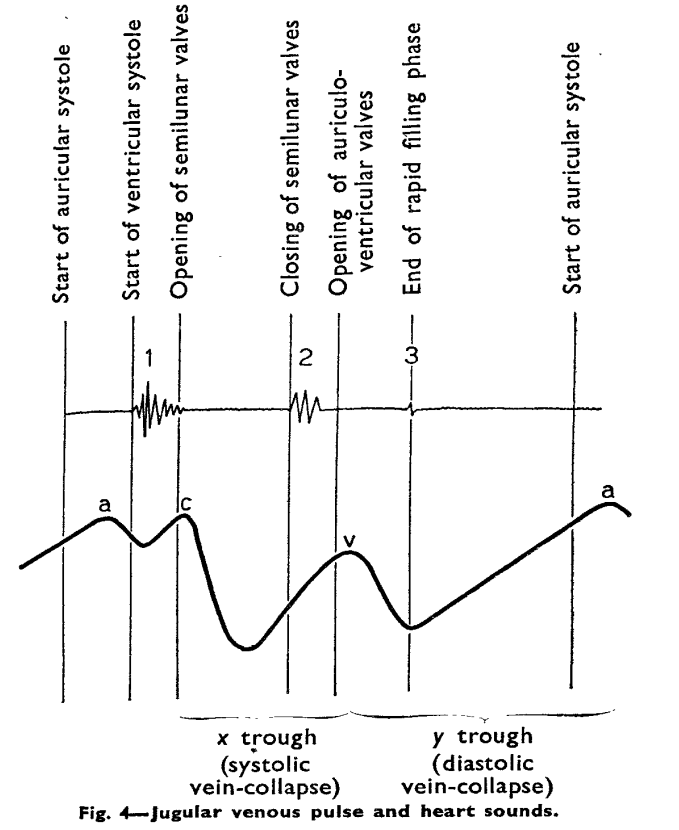
JVP typically has three positive waves and two negative waves. The “A” waves are due to atrial contraction while V waves are due to passive atrial filling. A waves are timed prior to S1 and V waves peak around S2. A tiny c wave interrupts the “x” descent . The word “c” could refer either to the RV contractile force or carotid contamination in the neck or simply a controversial wave.
The downward waves are X and Y descent. The major X descent is due to systolic atrial filling*, when the tricuspid valve is closed. Y descent is diastolic atrioventricular filling.
One interesting echocardiographic correlation has been observed. The force, power, and amplitude of X descent indirectly reflect RV contractility, and it can be referred to as poor man’s TAPSE.
One clinical question often asked in cardiology boards for fellows.
What are the difference between V waves that occur in ASD and Tricuspid regurgitation ?
V waves in ASD vs Tricuspid regurgitation
V wave is due to passive filling wave of atria when the ventricle is contracting and Tricuspid valve is closed.This physiological v wave . In ASD*, this wave just gets exaggerated as the right atrium receives the shunted blood from left atrium when the trisupid valve is closed. Since it almost resembles normal atrial flow pattern , both X descent and Y descent are retained ,and y may be slighly prominent in ASD.
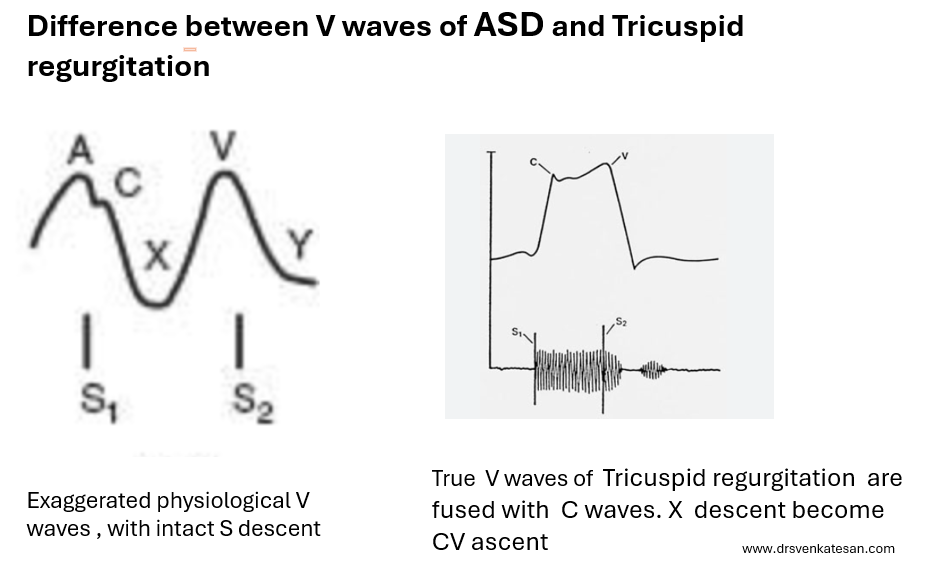
In Tricuspid regurgitation , the V waves are truly pathological in terms of opened tricuspid valve and timing of TR jet which fills the atria in systole rather thanin diastole. (Note this is different from the excessive diastolic filling of atria as in ASD )
While Y descent is prominent in both ASD and TR ,the X descent in TR is lost for simple reason. tricuspid valve is leaking and TR jet abolish the systolic X descend, rather it becomes a X-ascent (Conventionaly called CV waves)
*Please note, the v waves of ostium primum ASD, may not follow this rule as MR from cleft mitral valve further modifies the v wave.
Final message
When we analyse the V waves in JVP , it is important to assess its timing, relative to 2nd sound and also the both the descents to derive maximum hemodynamic information.
Reference



