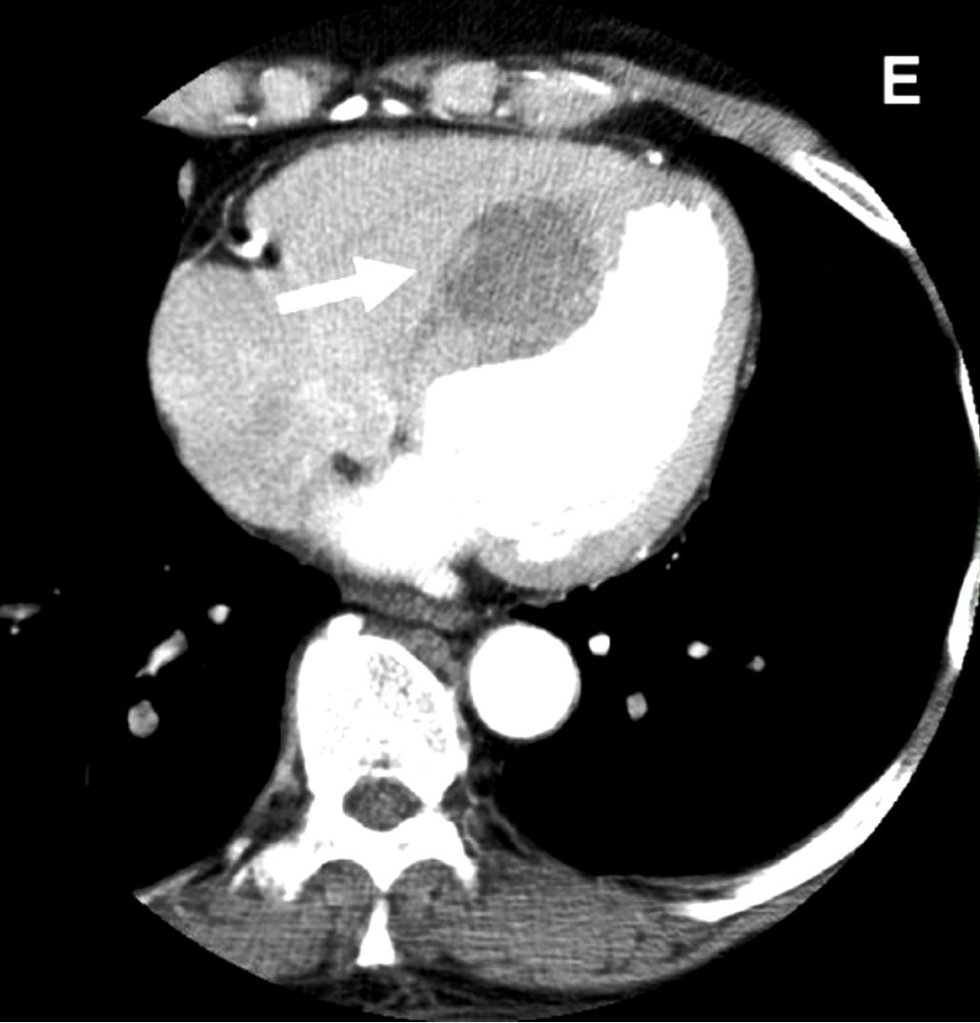
What is the lesion?
It looks like an Intracardiac tumor, a myxoma ? a variant of HCM ? Is it a hydatid cyst, ?
No it’s not. I can give one clue. This is a man-made condition.
Oh ok, did this happen inside the cath lab ?
Yes, you got it, right. But need a diagnosis.
Can you give me one more clue?
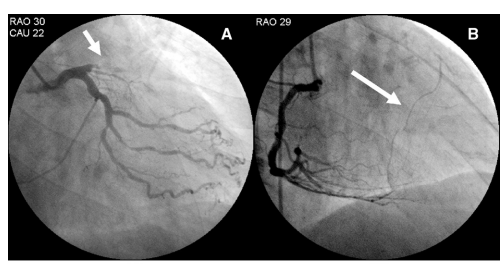
This patient was undergoing PCI for chronic total occlusion.
So, it must be a complication. Then I need to know the list of complications during CTO PCI.
Yes, but you may not find this one in the conventional list. Let me come out with the answer.
Answer
It is a huge septal hematoma due rupture of vulnerable septal collateral during retrograde wiring for opening LAD CTO.It usually occurs due to o prolonged procedures and hardware-related injury. Thanks to the authors from Taiwan to post this case report. (Image Courtesy Lin & Wu 2005 Ref 1)
Lessons from this case report (Not meant to offend anyone )
This case gives us some important lessons to be learned. One of my senior colleagues used to say, opening a CTO is ok, but using a retrograde approach with aggressive deploying of hardware within the last remaining lifeline provided by the donor coronary artery is a culpable coronary crime unless it is a life-saving procedure.
The often used term “septal surfing” adds an “adventure sport feel” to our youngsters posing as an interventional challenge and amplifying the potential injury. The fact that epicardial collaterals have a larger caliber, but the temptation to cross it, is significantly suppressed (or even forbidden) due to the risk of tamponade. However, this doesn’t in any way give us the freedom to toy with septal collaterals. Proliferating hardware (Innovative though ) is also an issue. It is true, technological input is a pillar for the growth of science. However, it is a sad fact, many of us are compelled to learn risky, unscrutinized tricks exclusively from academically unbaked industry guys, rather than from mainstream literature.
Final message
“No procedure … no complication”
I could recall, one of my colleagues displayed this caption as the last slide in a cath lab workshop, after a talk on How to avoid complications in the cath lab.
Very true. But, CTO by itself never belongs to a malignant subset of CAD, as some sections of the cardiology community would want us to believe. CTOs do need an intervention, only as a life-saving /0r severe symptom-relieving procedure. Most of them aren’t. They present with stable angina because of extensive collaterals. Unfortunately, instead of respecting this, many of us are asked to close these channels and try to maintain antegrade flow. The irony is, to open the CTO we may end up sacrificing these life-saving channels.
Reference



