ECG diagnosis any one can make. The second part of the question needs some thoughts.
Dissecting the ECG* diagnosis
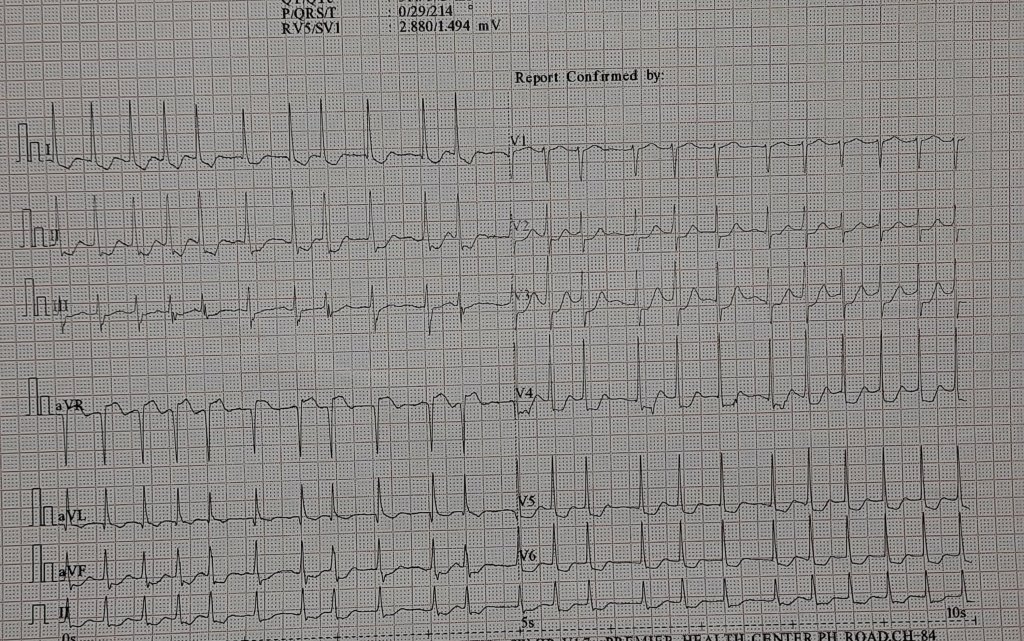
1.It is Atrial fibrillation with fast ventricular rate, with signifcant ST depression in V 4, V5, V6 .This could Indicate few things.
2.Preexisting LVH with AF
3.AF with new onset ST depression. This would mean an emergency (or may not) if it is an thromotic ACS high risk UA with posssible left main. But, one should bear in mind AF is an Natural atrial stress test , and ST depression could simply be a marker of tight fixed, stable lesion, (without a thrombus) that would require an elective Intervention.
4.Coming to the The ST elevation in AVR, many strongly believe it is a marker of left main disease. (Still, we can’t call it as AVR- STEMI, because it may just represent reciprocal ST elevation to any sort of ST depression in lead V5/V6 that includes benign LVH )
5.Look for ST elevation in lead V1 whenever you have ST lifts up in AVR. If V1 is isolectric , left main is very unlikely
The second part of the question.
I am sure, ruling out CAD without angiogram will be labeled as outright crazy. No cardiologist in their right sense will do that, I guess. Still, we could do it in this case. What did we forget in this discussion so far? We got lost in the electrical debate and failed to address the fundamentals. Why did this patient come to the hospital, requiring an ECG?
What did the clinical examination reveal?
While the cardiologist could not rule out CAD, the calm patient, complaining only of palpitations, ruled out a potential emergency chain reaction. Furthermore, a crescendo murmur in the aortic area sealed the issue. Yes, it is moderate aortic stenosis confirmed by an old GP’s prescription slip. She is being evaluated again for the severity of AS, treated with rate-controlling drugs for AF, since there was no acute heart failure or angina.
One more question
Why AF is not precipitating left heart failure even in patients with aortic stenosis ?
The concept of Left atrial functional reserve is a seperate topic, that will answer this query.
Final message
You don’t require an urgent cath lab mobilization to rule out CAD, even in a patient with a frightening ST segment, stuttering amongst irregular tachycardia. Always listen to the patient and have enough patience to look into the old records.. For that, we need to realize, we have to allow the patient to talk.
Postamble.
Presence of AS in no way rules out a CAD.Both can co exist. But if severe AS occurs with significant CAD, absence of angina is exceptional.



