Atrial fibrillation: Think locally act globally
It is clear, except in specific situations like HT, LVH, HFpEF, and other left (or right )sided structural heart diseases, the bulk of the AF is part of systemic destabilization of neuro-metabolic homeostasis. Atria become a poor, jittery victim to a complex interaction of multitude of factors like obesity, systemic inflammation, fatty infiltration, anxiety, abnormal neuro-cardiac modulation, chronic oxygen deprivation. etc. Of-course ,the final denominator is atrial stress. Though we have a strong bias towards left atrium, right atrium can equally be a culprit. Finally, apart from all the risk factor listed above , aging, is the biggest risk factor (Structural and Hemodynamic wear & tear ? )
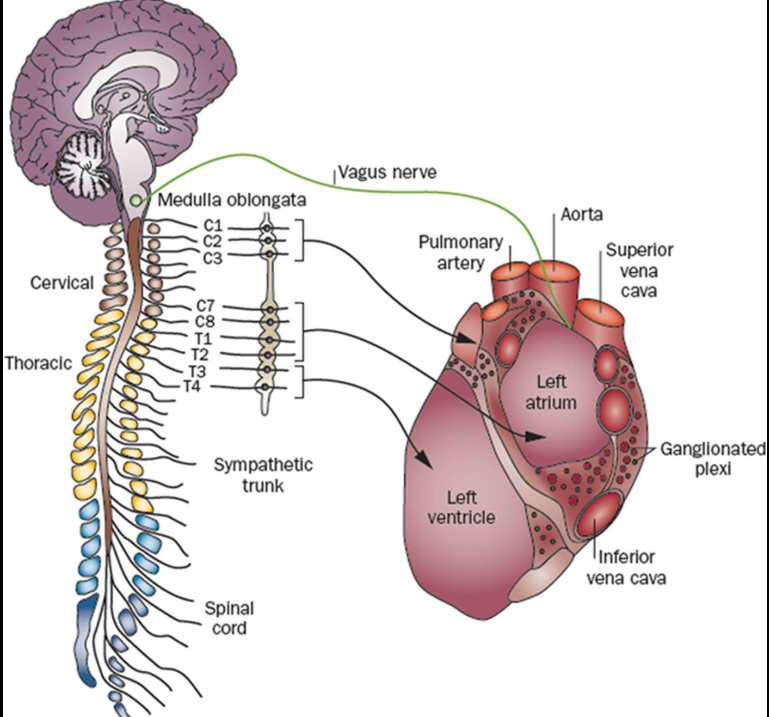
Probably, the most difficult question to any cardiologist, (however intelligent he or she may be) is this one. .Can you name and track all the nerves that supply the heart ? (While we can rattle all the coronary branches even in sleep)
Neurogenic origin
If we thought AF is more of adrenergic arrhytmia , we have equal evidence for it being vagotonic as well . The fact that , it occurs during episodes of emotional stress, both flight & fright reactions make it clear it’s catecholamine excess that includes dopamine,. Vagotonic AF occurs when extreme bradycardia releases subsidiary atrial ectopic activity, and a p on Ta waves and triggers an AF (like R on T for VT) Vagotonic AF in healthy athletes are reported confirming the existence of pause dependent AF similar to pause dependent VT VF.
Metabolic and Inflammatory
This emerging new factors point to fatty infiltration of atrium and subsequent fatty degeneration of atrial myocytes . The systemic player is the derangement of lipid metabolism as in obesity .Also, it is worth emphasizing ,the adverse effects of sub- epicardial fat is not confined to ventricle.(Al Chekakie MO, Akar JG. Epicardial Fat and Atrial Fibrillation: A Review. J Atr Fibrillation. 2012 Apr 4;4(6):483.) Left atrial adiposity is a distinct entity, but rarely diagnosed (.Circ Arrhythm Electrophysiol. 2010 Jun;3(3):230-6. )
Impact on AF therapeutics
We are in aggressive space age & AI era. AF management is no exception. For many us, frying or freezing the atrial or pulmonary venous tissue would come to our mind first , overlooking systemic factors. The obsession to restore sinus rhythm, persists in most of us, in spite of the RCTs showing clear equipoise between rate and rhythm control. We don’t need to think deep, to realize, modalities which take on this arrhythmia head-on has a minuscule role at the population level.
Simple measures, optimal BP, like weight reduction, (Atrial interstitial fat shedding) , relaxation can prevent 90% of AF burden. (Ahammed MR et al Impact of Weight Loss on Atrial Fibrillation. Cureus. 2023 Sep 29;15(9). Regarding pharmaco-therapy, the celebrated vintage days of anti-arrhythmic drugs have almost gone. I don’t think any new anti-arrhythmic drugs are in the pipeline. Last being almost 4 decades ago (Ibutilide ?). Theoretically, (& realistically) most of the drugs in all the four sub class of W&W drugs can be effective in AF .
Currently, one thing is striking, (at-least to me) .Beta blockers seems to be under utilized in AF (Amiodarone took over the AF arena like a Don, two decades three decades ago, still surviving, despite the side-effects ). A beta blocker in adequate doses will definitely control most forms of AF , especially the lonely neurogenic ones which form the majority.
Some EPs do hail sotalol, not because it is a beta blocker but because it mimics Amiodarone with a class 3 action. A big plus for BBs is it is welcome even in the presence of LV dysfunction. It possibly has a central anti-adrenergic action modulating the neuro-cardiogenic function. One issue with BB could be ,it is to be used with caution, if AF is an accompaniment of sinus node dysfunction.
Final message
AF is probably the most common cardiac arrhythmia, and many cardiologists believe they have exclusive rights to handle it .The reality is , in terms of etiology and triggers AF lies elsewhere outside the field of cardiology. Any good physician can easily recognize and manage this arrhythmia with simple measures, advices and liberal use of beta blockers, without the need of tricky drugs like Amiodarone . Invasive ablation procedure are reserved for a fraction of the population. Unfortunately, modern science seems to worried more about this small subset and keep throwing exotic discoveries ,diverting our senses.
Reference
How many of us know there is a journal exclusive dedicated to AF ? Journal of atrial fibrillation



