OCT, the magical intraluminal coronary vision, has been a great innovation that helps us to decode many uncertainties in the morphology, behavior and vulnerability of coronary plaques. It is used widely in pre- or post-PCI or even asssit during the implantation of stents. The role of OCT/IVUS is sometimes deemed critical in dealing with left main and bifurcation lesions.
Of course, there were some overuse of OCT as well, as many centers did it for some academic fun, even in some innocuous lesions. Meanwhile, there is a striking miss. We probably failed to accrue the benefits of this revolutionary imaging in the graft evaluation. Its real role could be in LIMA grafts including anastomotic site or SVG lesions in the immediate postoperative or at long-term follow-up lesions. As far as I understand, it is very rare for cardiologists to attempt imaging these sophisticated tools in LIMA or SVG.
Published data on OCT IN LIMA
Here is a paper from a stalwart in coronary interventions, Dr. Patrick Serruys and his team from the Netherlands (Published in 2009 ,but surprised to find not many takers)

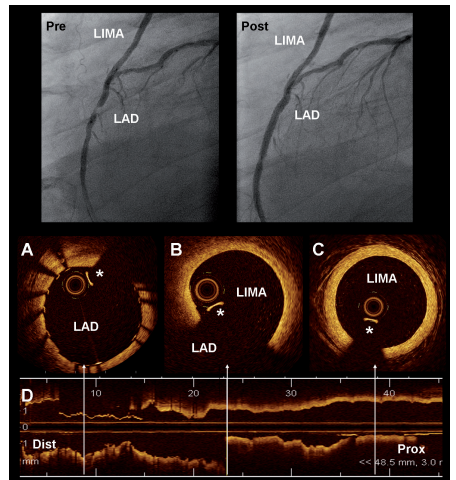
Image source & Courtesey : Ref 1 Optical coherence tomography (OCT) visualisation of left internal mammary artery (LIMA). The superior panel shows the angiogram of a patient with a graft of LIMA to the LAD.
Why OCT/IVUS is less popular in graft assessment ?
*Graft follow-up often falls under surgeon’s domain. They don’t call for check angio often, unless the patient is really, really symptomatic. (CT angiogram is more popular in post CABG)
*From cardiologist’s point of view, they rarely deem it to be necessary. Reason being, it could be technical (Will the venous graft tolerate the OCT wires?)
*Lack of experience and apprehension
*Lack of publsihed data.
Final messge
It is true, doing regular graft angiogram, by itself is less than 5-10 % of all angiograms . Asking for OCT in that population is big deal .Still, OCT can be a valuable in providing crucial information in the assessment of both LIMA and SVG, at least in the former. One more purpose of OCT is, its offline use to assess the integrity of LIMA graft on table prior to CABG. It can confirm patency and possibly rule out any significant takedown injury, that is missed otherwise.
Reference



