We know, stress tests can give false positive results suggesting ischemia in at least 20% of patients for various reasons . It can occur with systemic (Anemia) and cardiac conditions such as HT, LVH, baseline ECG changes, or myocardial disease.
Here is a middle-aged man who went for an annual health check and ended up with this TMT. His exercise capacity was good at 11 METs, stopped at early stage 4 standard Bruce. He was asymptomatic, and every other parameter was normal.
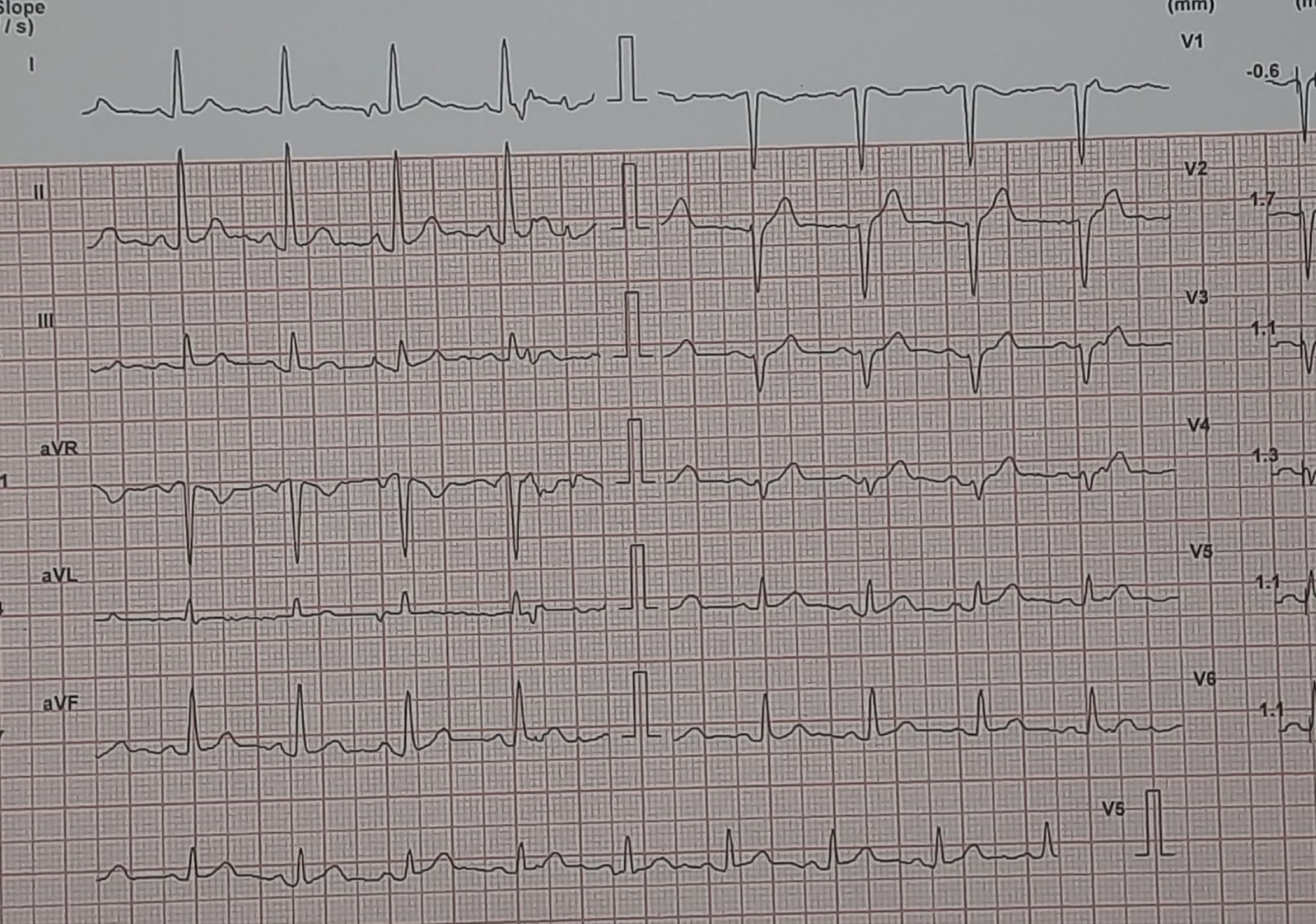
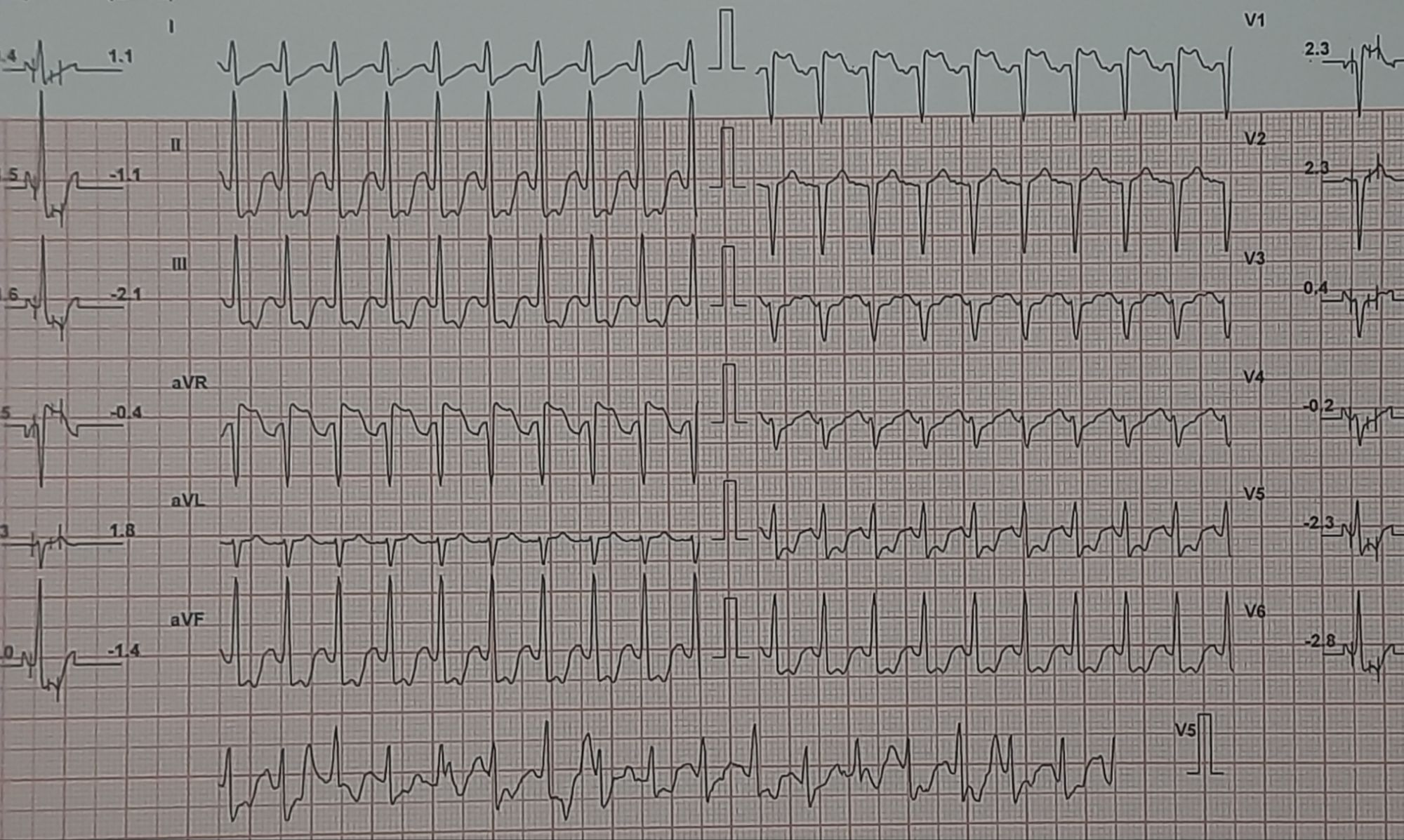
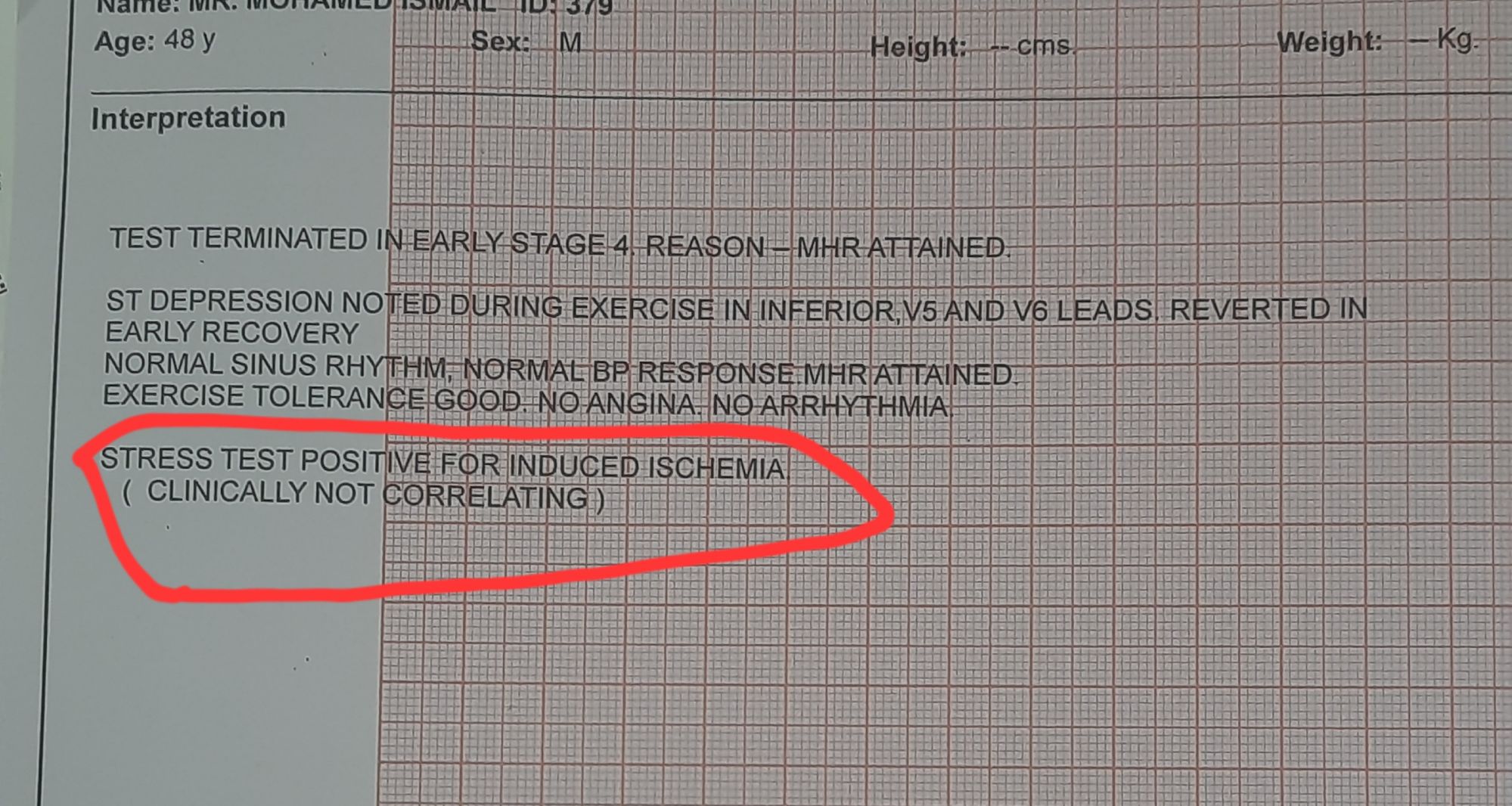
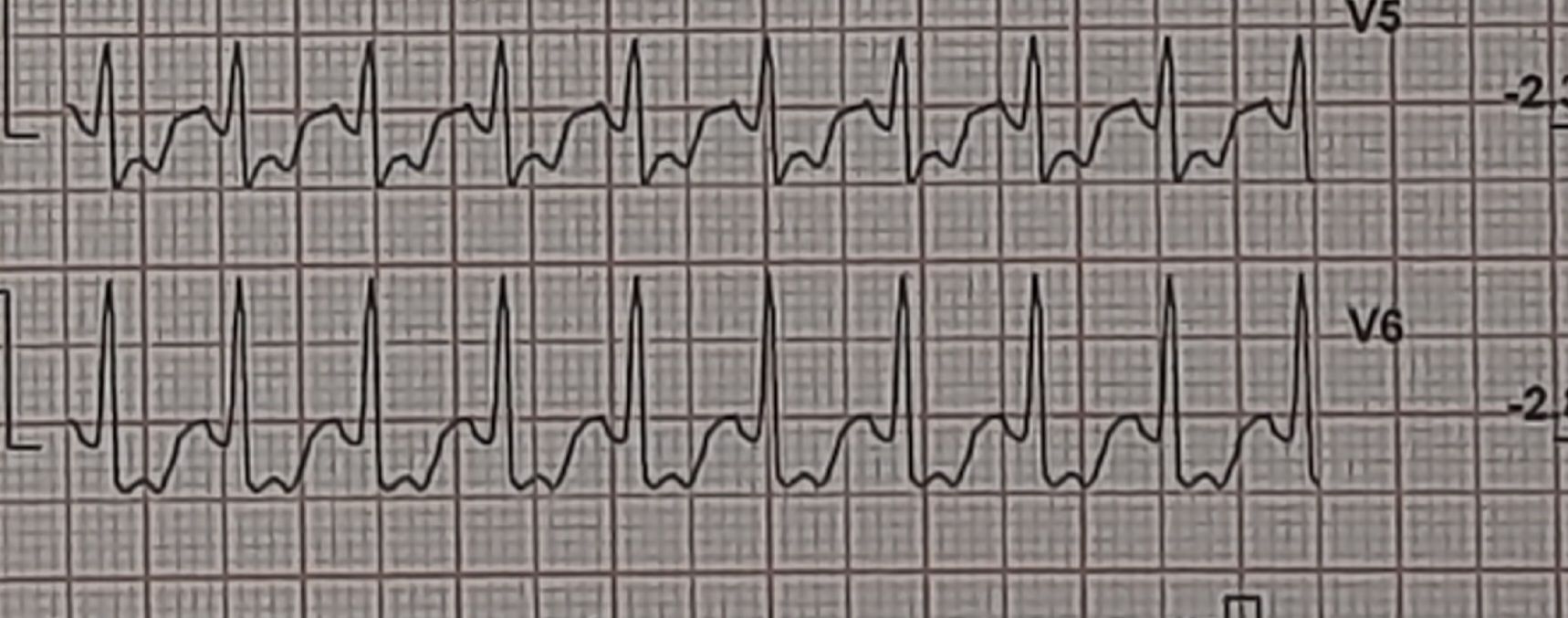
Images: Resting, Peak, severe positive response, in lead V5 and V6. Every cardiologist advised some form of CAG. Opinions were so diverse, ranging between silent left main, tight proximal LAD to innocuous false positive.
What is your inference ? The patient seeked by advice It was indeed an academic stress test. There is a frightening ST depression I said. yes the rest is very likely to be false positive but I don’t have the courage to commit so. Mostly, you can’t escape from a coronary angiogram” . Next option is CT angiogram, Thallium or dobutamine stress.
It was indeed an academic stress test. There is a frightening ST depression . Very difficult to Ignore. May be, it could be false positive but I don’t have the courage to commit so. Mostly, you can’t escape from a coronary angiogram” .Other options are CT angiogram, Thallium or dobutamine stress.
He smiled and said, “You are absolutely right, doctor. Out of 5 cardiologists I consulted, 4 asked me to go for an immediate angiogram. Still, I escaped because of one Egyptian cardiologist.”
I was eager to see what he did . This is the test he did.
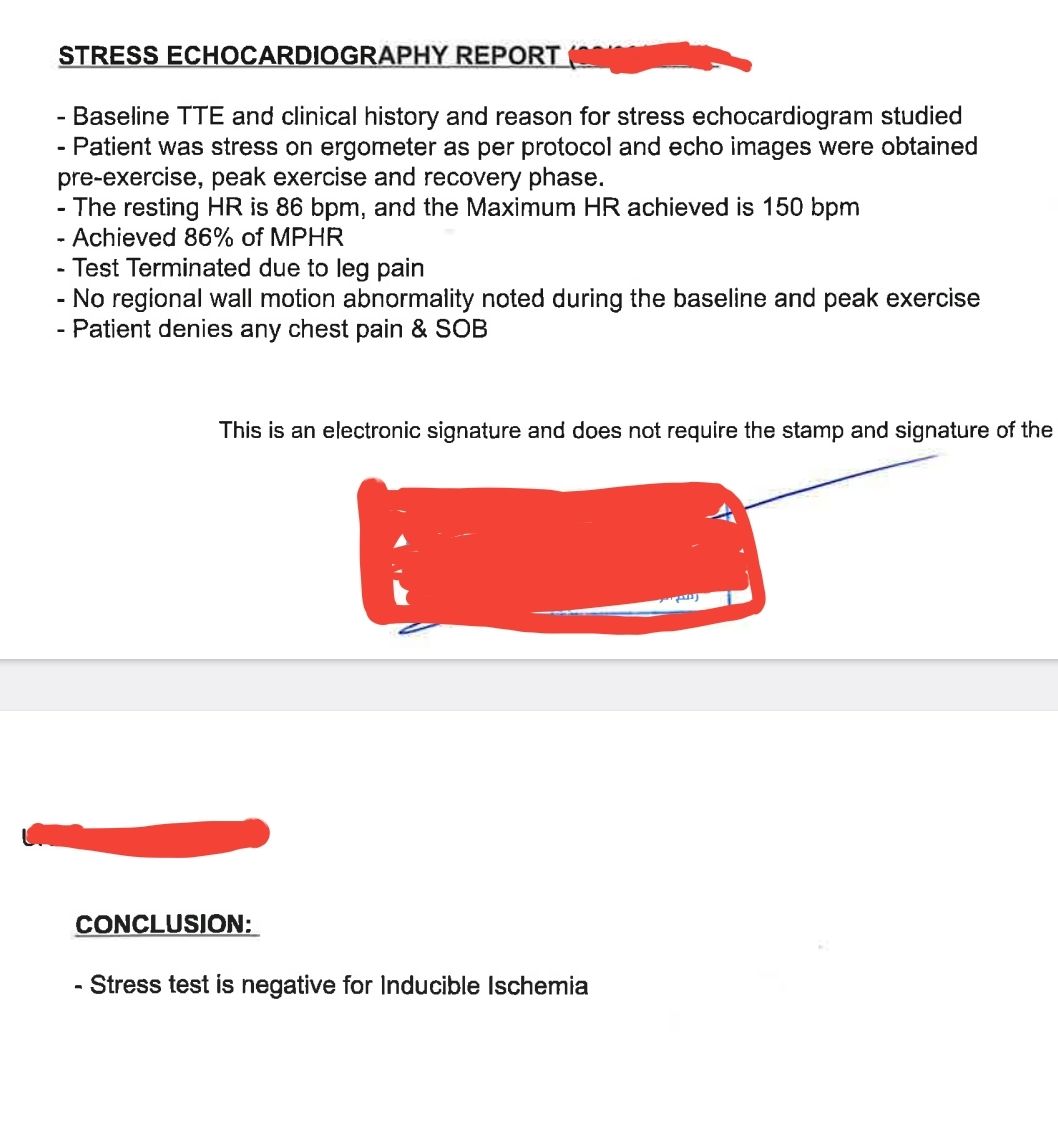
Yes. It was indeed a smart move. The shrewd cardiologist did a bicycle ergometry and simultaneous echocardiogram without any drugs or injections. He could confidently rule out significant CAD (by absence of any wall motion defect). Hats off to him. Lets earn some courage from such truely learnt cardiologist.
Final message
Most of us (Cardiologists) find it difficult to trust the physiological data that come from history, ie excercise capcity . We are obsessed with anatomy. Though, we eloborately debate about physiology-based intervention inside cathlab in every conference.
Our flawed intellect keeps asking this question: How can I trust physiology (Flow) without documenting a good anatomy? In fact, truth is the other way around. A good epicardial anatomy rarely guarantee good physiology. (It is worth recalling, CAG, the investigation we celebrate as the gold standard, images only about 2% of the entire coronary vasculature.)
A well-documented near physiologically flowing coronary circulation, negates the need to document anatomy through whihc it flows,however shabby or good it may be. (For the FFR & iFR guys, it must be mentioned that a negative stress test implies a net combined three-vessel FFR of > 0.9.)
Postamble
There was a well-accepted holistic, yet scientific concept roaming around in cardiology academic circles in the 1990s. (Of course, now it is thrown to the dustbin.) It said, if anybody crosses 10 METs in TMT, he or she is unlikely to harbor a significant lesion; even if there is one, it usually doesn’t require a metallic fix.



