The answer is, yes, but a crude yes. A lot of OCT literature has taken this aspect casually. Macrophages, both resident and blood borne monocyte-macrophage, lay the foundation for the athersclerotic plaques. Currently, cardiology imaging specialists tell us, that bright spots in OCT, beneath the Intima are believed to be macrophages, based on a few histological correlation studies. If you go through these studies (Ref 1), it is almost guessing like tossing a coin .It finds 57% of bright spots were macrophages. The rest 43 % can be any of the following 7 in the list.
The causes of bright spots in OCT are too many
1.Lipid Pools/Necrotic Core: Lipid-rich areas or necrotic cores in plaques can appear as hyperreflective spots.These may mimic macrophage infiltration but are typically larger and less discrete.
2.Cholesterol Crystals: Resemble macrophage-related foci but are often linear or needle-like.
3.Calcifications: We know calcium is always a bright spotin any Imaging. Same with OCT Microcalcifications or early calcium deposits in plaques can appear as bright easily mistake formacrophage. But, unlike macrophages, calcifications are often accompanied by acoustic shadowing.
4.Fibrous Tissue: Dense fibrous tissue in stable plaques may occasionally produce bright spots, particularly if imaging artifacts enhance their reflectivity.
5.Neovascularization: Reflection due to red blood cell content or vessel wall components, mimick macrophage accumulation.
6.Thrombus: Small thrombi (red or white) within plaques can appear as bright spots.
7.Imaging Artifacts: Motion artifacts, stent strut reflections, or incomplete blood clearing during OCT imaging can produce spurious hyperreflective spots that mimic macrophages.
Please note :The most important factor in the above list, is the last one, ie technical and Imaging artifact.
Can we identify true macrohoages with emerging technologies ?
We are in the era of virtual histology. It may come true in the future. Current generation OCTs have 10 to 20 micron resolution.
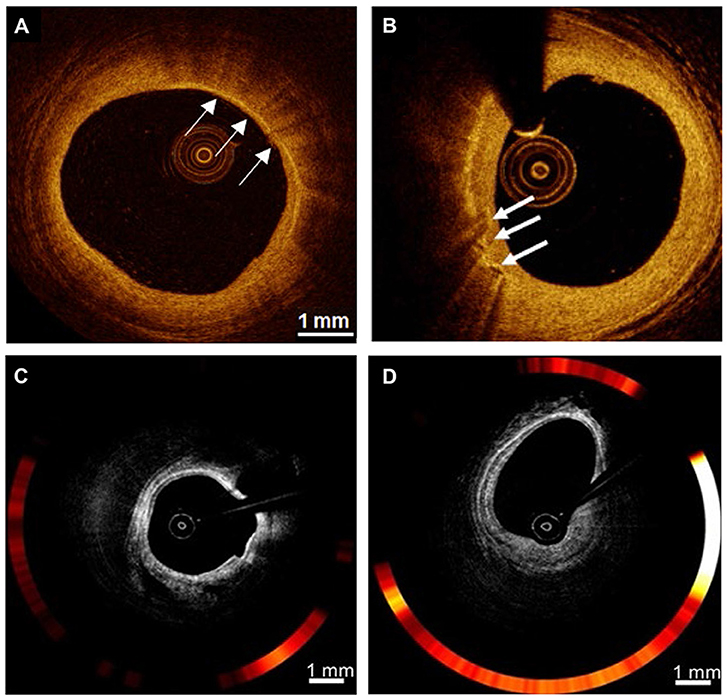
Image source (Ref 2)OCT cross-section images of the atherosclerotic vessel lumen, the location indicated by the white arrow is, rather susspected the macrophage. (C,D)
Advanced techniques like USPIO*-enhanced OCT and μOCT** show promise for more precise macrophage detection, but they are not yet standard in clinical practice. For now, OCT remains a valuable tool for assessing plaque vulnerability, in which we believe macrophages are playing a key trigger.
*USPIO: ultra-small superparamagnetic particles of iron oxide (USPIOs) is an MRI contrast agent
What is purpose of identifying these macrophages with such costly technology?
Not much really. May be a feel of scientific enthrallment. Of course, it can help monitor plaque healing, which is going to happen anyway whether we visulaize it or not if proper medications are taken (Intensive dose statin). Ofcoure ,these imaging modes do have a role , if we want to know how the macrophages are going to feed on the bio-absorbable stents.
Final message
All that blinks bright in OCT, are not macrophages. Virtual histology-based interventions are great scientific tools, but have little value in cath lab interventions as of now.
Reference
Follow up question
Do the macrophages invade the stent metal ?
The answer is an unequivocal yes. The catch is, DES , tends to whip out the macrophages from its vicinty . BMS welcomes it . Which is good ? Think about it , answer will be very surprising.



