This is not a completely Imaginary conversation, between the wife of a recently discharged STEMI patient and his cardiologist. This happened in a top ranked heart care center in my city Chennai.
Caution: Strong language
Patient’s wife :
Doctor, why my husband is suffering from significant LV dysfunction in spite of a timely & successful primary PCI. You assured me you are doing the best.
Cardiologist:
Yes, you are right. I am sorry, for that.
Patient’s wife :
But, doctor, on the day of discharge you told us proudly, the procedure is 100% success and you have relieved the block and restored blood flow. I recall, you quoted some Tomy score, and all.
Cardiologist:
Yes I did. It is not Tomy, it is TIMI 3, which we use routinely, and … to be frank, it actually means nothing. It tells us, we have restored flow across the artery at the site of block . It can never guarantee, all those blood, will reach the ailing muscle.
Patient’ wife:
TIMI or TAMY, doesn’t mean anything to me doctor, It sounds like my neighbors’ pet. All I want to understand is , whether the procedure was really successful. Yes or No ?
Cardiologist:
You are correct. I am extremely sorry. It is really an Incomplete myocardial salvage. Your husband’s myocardium is significantly damaged. You must also understand , these things are not in our hands. It is the destiny that decides the fate of the myocardium. It lies deep in the myocardial microvasculature, which doesn’t obey our conventional time windows we talk about.
Patient’s wife:
That’s ok. But, what is the need for mis-communication to us. Why didn’t you admit it as a failed primary PCI in your discharge records ?
Cardiologist:
I agree with you. But, scientifically it is not a falsehood. For us, it is still a success, because we are just macro-vascular cardiologist. We define success based on removing blocks, not the true myocardial reperfusion.
Patients wife:
That’s awful. Sorry, for being harsh .For heaven’s sake please go and change your horrible definition for a successful PCI ,in the cardiology literature.
Cardiologist:
Thanks for bringing up this less discussed entity “Failed primary PCI” We rarely discuss about it (In the biased minds of interventional cardiologists, only thrombolysis can fail). Surely, we will pass on your genuine concern to the concerned authorities.
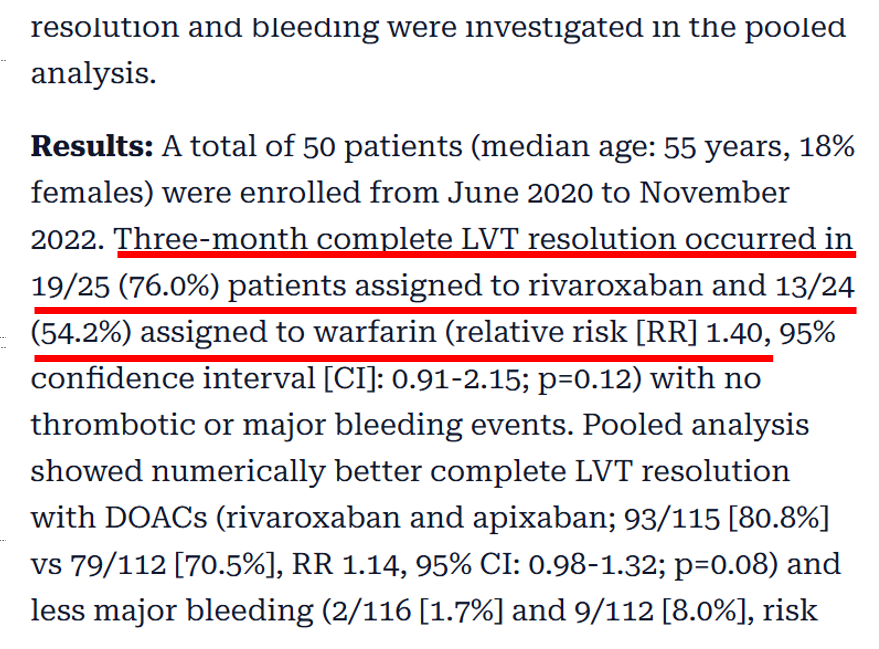
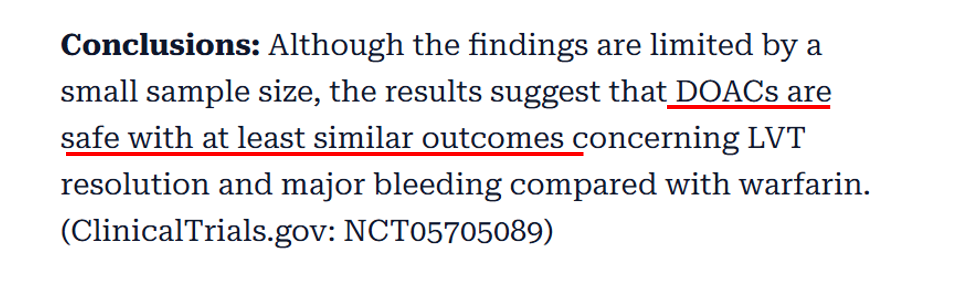
DoesDOACs trying to push over warfarin in post STEMI LV mural thrombus ?
Yes , it seems so. Old must give way for new, even if it is gold. We need to go with the trend. Only thing, we need to prove is, whether the new ones are safe . Need not bother much about efficacy. Some one, will somehow, prove the new ones , non-Inferior to the best available drug as on date.
Every experienced cardiologist would know, Warfarin is many-fold more effective. But, still NOACs are coming in a big way. With the help of big trials, NOACs will ultimately replace the much more dangerous, bleed-prone Warfarin. One more reason we might embrace the inferior drug is the clinical inertia for vigilant INR monitoring.
What does the evidence say ?
Read : Ref 2
The future of medicine will be fight between quality & ( Intention ) of evidence and experience
Caution : Personal opinion
It would be science at its best, when a less potent drug, that requires zero monitoring, will replace a more potent and established OAC. It doesn’t require brilliant brains, to realize a drug which has less bleeding risk, is going to be less effective in getting rid of thrombus as well. (The trial in Ref 2 proved otherwise)
Only issue with warfarin is, we need to be a little more careful. Fortunately, its usage in LV mural thrombi is not likely to be permanent. (as in prosthetic valve)
Reference
AHA comprehensive review on LV thrombus management
Innovation and Interventional cardiology are like Inseparable conjoined kids. When a mind blowing idea shakes hands with unprecedented technology, supported by an accommodating industry, such breakthroughs happen.
First In human : Creation of neo-coronary ostium & by pass stent to LAD
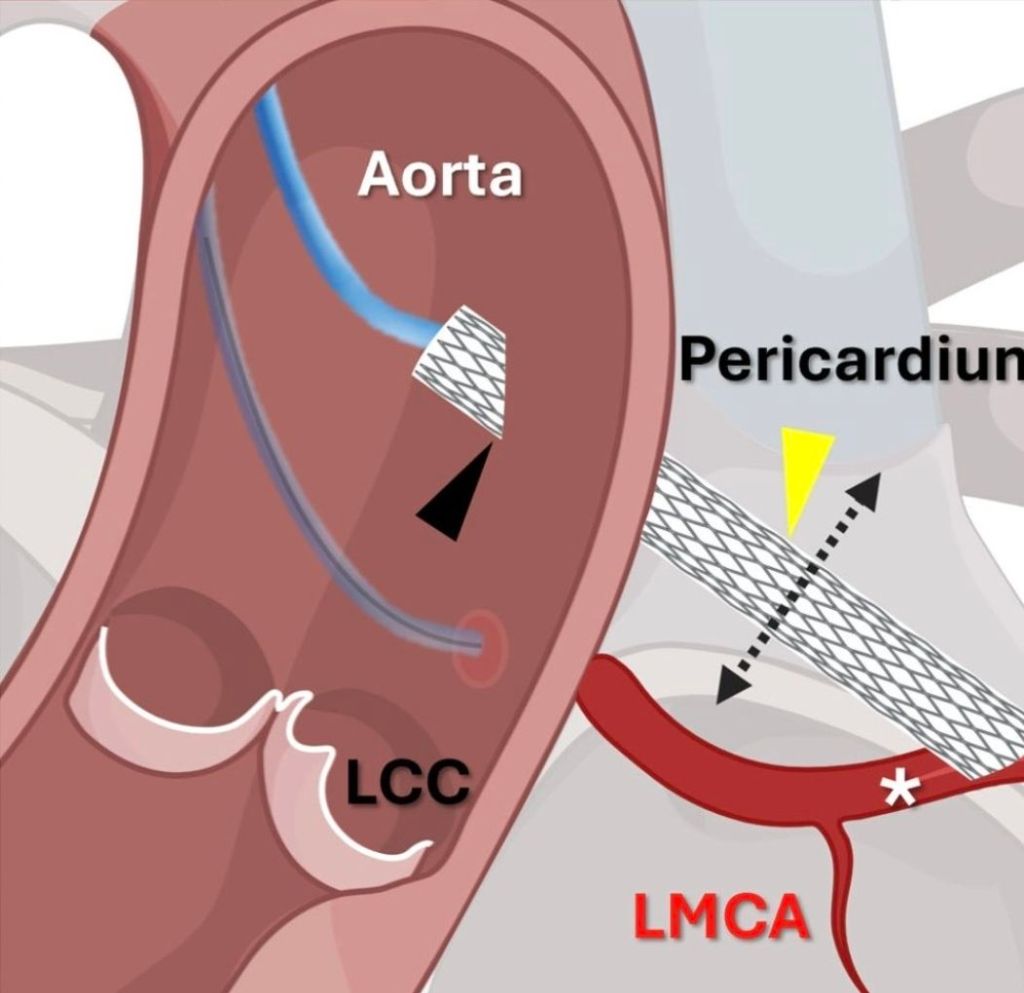
Here is an ultimate intervention, called the VECTOR procedure, that creates a tunneling pathway outside the regular anatomical pathways, like laying a road or metro tunnel under a mountain or river. (Ref 1 Circulation Cardiovascular Intervention 2026)
Combining the expertise of the retrograde approach of CTO and covered stent technology, a neo coronary ostium and an artificial artery is created that connects the ascending aorta and LAD, burrowing through the epicardium, myocardium, and pericardial plane.
A very high risk post TAVR, who had a blocked his left coronary ostium. VECTOR was attempted in lieu of CABG, which probably he was not eligible.
2.Where it was done ?
I think it was done at Emory , the same place Andreas Gruentzig, show cased his magnum opus.
(It is a combined innovation from four institutes Structural Heart and Valve Center, Emory University Hospital, Atlanta, National Heart, Lung and Blood Institute, National Institutes of Health, Bethesda, St Francis Hospital and Heart Center, NY, MedStar Washington Hospital Center and Georgetown University, Washington, DC0
3.What are possible percutaneous solutions to prevent coronary ostial obstruction ?
1.BASILICA (Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction)
2.UNICORN (Undermining Iatrogenic Coronary Obstruction With Radiofrequency Needle)
3.CATHEDRAL (CATHeter Electrosurgical Debulking and RemovAL)
The VECTOR procedure , first in human human was attempted
4.Now, what are challenges ? Will such procedure stand the test of time ?
The key question is, (apart from complexities and complications of the VECTOR procedure) how the covered stent will seal the peri-anastomotic site both in the aorta and coronary end?
5.Is this procedure possible in a non-TAVR situation in complex ostial and left main disease?
If we can, somehow make the procedure simple with smaller hardware, circumventing VECTOR will be an ultimate victory for mankind and sure to stand tall in the pinnacles of glory.
However , when adopting new technologies “Always be ready, to sacrifice science , if you think it would interfere with patient well being”.
Cardio-renal syndrome (CRS) , in reality seems to be , a vague clinical entity, defined and classified into 5 types essentially for our convenience and simplicity. This classification do not contribute to any pathophysiological insights . The fact of the matter is, every patient with heart failure (both acute and chronic) has some amount of renal compromise & vice versa. The link between LV failure and renal compromise is more discussed and documented in the literature than the influence of the right ventricle.
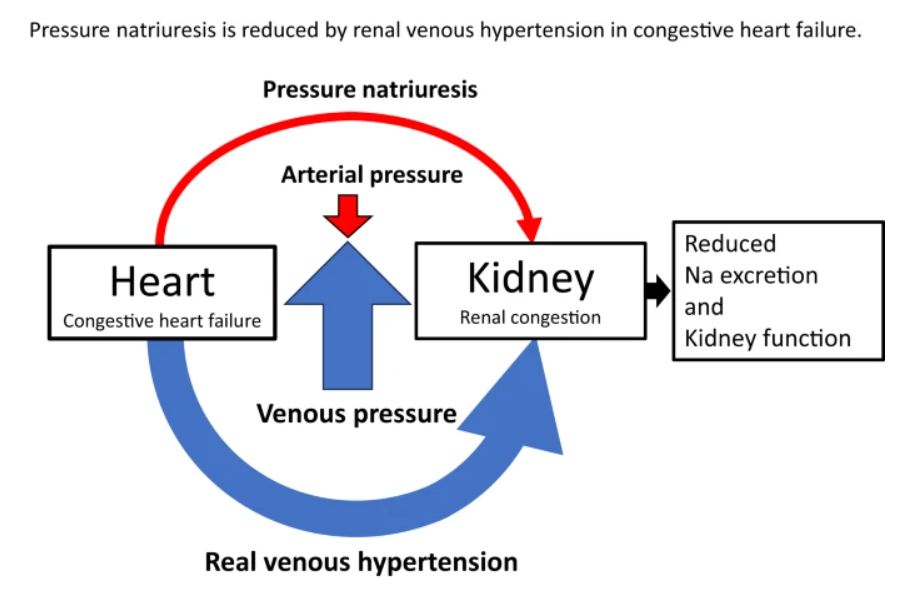
Now evidence is emerging, like hepatic congestion , renal venous congestion also play an important role in compromising renal function. Traditionally, we aim to increase the GFR, by improving renal blood flow, but the real problem may lie in clearing the exit paths of the renal venous system.
A mini review on the topic
Right ventricular (RV) dysfunction in chronic heart failure (HF) contributes to renal dysfunction beyond reduced forward cardiac output, primarily through backward venous congestion elevating inferior vena cava (IVC) pressure and renal venous hypertension. This congestion transmits high central venous pressure (CVP) to renal veins, increasing interstitial pressure, compressing tubules, and impairing glomerular filtration rate (GFR) independent of arterial underperfusion. Studies confirm IVC dilatation and CVP >8 mmHg correlate with worsened renal function, reversible by decongestion.
Venous Congestion Mechanisms
Elevated RV filling pressures cause systemic congestion, reducing trans-renal perfusion pressure (mean arterial pressure minus CVP) and promoting renal parenchymal hypoxia. Animal models show renal venous pressure elevation decreases urine output and GFR more than equivalent arterial hypotension, via tubulo-glomerular feedback disruption and renin-angiotensin-aldosterone system activation. Human data from acute decompensated HF link high RAP/CVP to serum creatinine rise, with decongestion improving GFR in RV failure.
Major implication is the role of optimizing diuretic dose in HF, which can reduce renal venous congestion . Treatment strategies aiming to improve pulmonary hypertension and RV function seems important as well.
Final message
If we need to manage cardio-renal syndrome effectively, we need to pull both Cardiologists and Nephrologists to sit in a combined consultation (a difficult proposition in current times), and review patient data, optimizing the strengths and weaknesses of all pillars of heart failure drugs, and (more importantly) fine-tuning the important fifth pillar, the diuretics*.
*For some reason, the literature and cardiology community refuses to admit a blatant truth : Diuretics are life-saving in heart failure.
The lubs and dubs, along with some added sounds are the only language, the heart can speak in health and distress. It’s a worrying story altogether, gradually many of us are becoming “cardiac illiterates” as we struggle to read , its gentle communication. it is not our fault. Stethoscopes are reduced to become a social marker of being a doctor. We may excuse ourselves, even if we can’t differentiate a systolic from diastolic murmur, after all, hand held echo machines, instantly tell the diagnosis.
( After reading this article, fellows are expected to understand why the first heart sound in MR (ie the lubs,) are mostly soft, some times normal or even loud in certain conditions)
Now, let us go to the mitral valve dynamics
How many of us are aware, there is a big science of physics and biology operating when the mitral valve perfectly closes at the level of the annulus, with each systole , balancing different sets of known and unknown forces.
In this article, we will see how these two sets of forces mitral valve tethering and closing forces balance out each other to seal the mitral valve and what happens when the forces begin to fight each other.
Balance of Tethering and Closing Forces in Mitral Valve Coaptation
The mitral valve (MV) coaptation refers to the edge-to-edge apposition of the anterior and posterior leaflets during systole, ensuring a competent seal to prevent regurgitation. This process is governed by a delicate balance between tethering forces (which restrain leaflet motion to prevent prolapse into the left atrium) and closing forces (which approximate the leaflets for sealing).
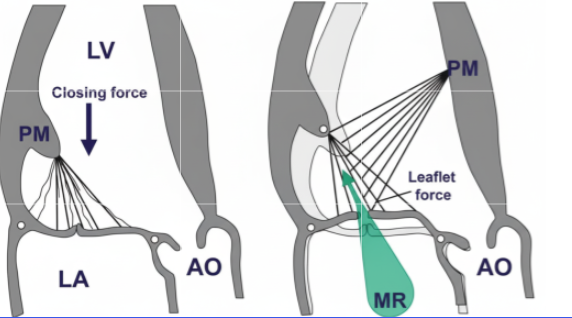
Tethering forces: These are primarily transmitted through the chordae tendineae from the papillary muscles (PMs) to the leaflet free edges and bellies, pulling the leaflets apically and laterally toward the left ventricular (LV) apex. They arise from:
Closing forces: These are driven by the transmitral pressure gradient during systole, where rising LV pressure (generated by LV contraction) exceeds left atrial (LA) pressure, pushing the leaflets together. The force is proportional to the LV dP/dt (rate of pressure rise) and peaks in midsystole.
Balancing mechanism: Coaptation occurs when closing forces overcome tethering, enabling leaflets to meet with sufficient overlap (coaptation length >8 mm typically). Imbalance favors regurgitation: excessive tethering (e.g., from PM displacement) causes apical tenting and incomplete closure; insufficient closing (e.g., low LV contractility) fails to seal the orifice. In health, the forces are synchronized with systole, with closing forces dominating midsystole to minimize the effective regurgitant orifice area (EROA).
Paradoxes in the Balancing Mechanism
MV mechanics exhibit several counterintuitive paradoxes, where adaptive or dysfunctional responses lead to outcomes opposite to expectations. These highlight the interplay of geometry, contractility, and force transmission:
Paradoxical systolic PM elongation: Normally, PMs shorten during systole (1 cm) to offset annular descent and maintain annulopapillary balance. Post-myocardial infarction (MI), scarred or ischemic PMs paradoxically elongate driven by transmitral pressure tension. This decreases annulopapillary distance, attenuates tethering, and reduces MR severity—contrary to the intuition that PM weakness worsens regurgitation. However, extreme elongation risks leaflet prolapse, flipping the paradox to increased MR.
PM dysfunction attenuating ischemic MR: In isolated dysfunction, reduced PM contraction intuitively increases slack chordae and prolapse risk. Yet, in localized basal inferior LV remodeling, PM dysfunction (measured as reduced longitudinal systolic strain) inversely correlates with MR fraction attenuating MR by limiting excessive tethering. This holds only with certain level of remodeling . Gross and asymmetrical remodeling can exaggerate tethering and increase the MR.
Dynamic EROA reduction despite peak driving pressure: MR often peaks early systole (when closing forces are low and tethering dominates) but paradoxically decreases midsystole, even as LV pressure (driving force) maximizes. This occurs because rising closing forces (transmitral gradient) overcome tethering, shrinking the orifice mimicking reduced regurgitation when it should worsen.Thgis mechansim can some times seen when MR jet is bi-fid in doppler tracing.
Imbalanced chordal forces causing focal prolapse: In acute ischemic MR (e.g., posterior wall ischemia), tethering redistributes unevenly: tension drops in ischemic-side chordae but rises on the nonischemic side causing focal tenting and relative prolapse on the ischemic commissure. This creates an eccentric jet despite global LV contraction.
This article clearly tells us that the forces acting on the mitral valve apparatus are so complex. The conceptual model of tethering and closing forces may be oversimplified. There are variable interactions between them. More importantly, the atrial forces also influence and intrude into these forces. Realize that MV competence is not just about force magnitude but their vectorial distribution and timing, often amplified by LV geometry changes.
Final message
As cardiologists and surgeons, we must realize the fact, how important it is to analyze both anatomy and the physiological impact when we rush to clip, cut, or repair it with annuloplasty and subvalvular interventions.
*Sometimes, it might even be tempting to do mitral valve replacement, even when it is not indicated, because we need not bother about all these dizzy mechanics and physics of MR jet forces.
As we enter, another customary happy “New year” , a lingering “Old wish” remains largely unfulfilled. Let us try to return, to our forgotten home space, called patient’s bed side . Shall get Immersed in history taking , Intuitive clinical examination, and master the art of listening to our patient’s heart with our own ears. Investigations can wait unless it is a dire emergency.
Too often today, we bypass these foundations, relying blindly on Images, echocardiograms, angiograms, a deluge of scans, , multi-modality algorithms ,AI predictions. We have also become greedy servants to technology commerce , and increasingly intoxicating science as well. Let us not insist on investigations , driven by peer pressures or pride, in the process losing common sense in a flood of data.
Let us reclaim the intellect, that taught us listening and understanding to the patients symptoms (with kindness) is the highest form of Investigation .
Coming to scientific research, grow courage to question, debate , that ultimately would simplify complex problems .
Finally, seek the truth, which often hides behind the distorted evidence base and obsessive compulsive protocols.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.







{kind=link}
{kind=link}
{kind=link}