PV isolation or ablation is considered as a ingenious and poular modality in tackling chronic recurrent AF. Still, it is too invasive and complication-prone, with less than desired success rates. EPs are struggling to mitigate the adverse events. Hardware has vastly improved. We have since moved from RF , cryo , to pulse field ablations.
Whatever said, AF is a chaotic arrhythmia. When we try to take on the chaos head-on with more force, considerable damage, mostly invisible, is expected in the atrial battlefield. One such thing is post-ablation atrial tachycardia. The exact incidence is under-reported. Many times EPs don’t consider this as a complication at all. It is funny, some percieve it as a partial success as as the chaos has become less intense. The fact of the matter is, an AT can carry more unpredictable and carry electrical morbidity with the risk of further AF always remain.
Incidence of AT post AF ablation
Organized atrial tachycardias (ATs) occur in 5–40% of patients after catheter ablation for atrial fibrillation (AF), with the exact rate depending on the index procedure strategy, AF duration, LA size, and follow-up duration.
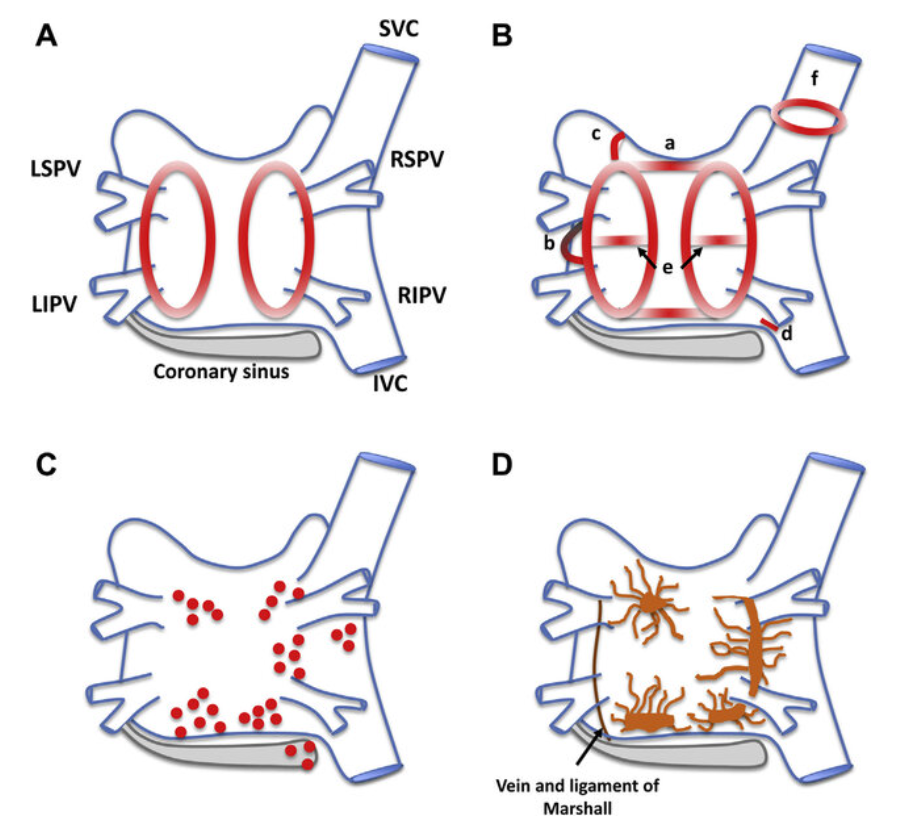
- With pulmonary vein isolation (PVI) alone: Incidence is lower (5% or less). When AT occurs, it is frequently focal, most often originating from reconnected PVs
- With additional substrate modification (linear lesions, complex fractionated atrial electrogram ablation, etc., common in persistent AF): Incidence rises to a prohibitive 20–50%.
- Macro-reentrant ATs also occurs due to gap-related peri-mitral or roof-dependent circuits.
Final message
Both focal and non focal ATs post-AF ablation are much common than we realise.Very often, they require another procedure or more intensive drugs . Realsitically, the real purpose of treating the chronic AF is lost , if AF is likely to be transfomed to focal or non focal AT.There is nothing called 50% chaos reduction in AF treatemnt.



