Recently , a young celebrity lost his life during gym session suddenly . The media erupted as expected .Every TV channel became a temporary schools of advanced cardiology . It seemed anchors knew more cardiology than us.
Among the peers, so many hypothesis were going around. The loudest one was prolonged QT. We are discussing a relatively new, (rather les popular ) entity for the potential cause of SCD. What is it ? DID is the new buzzword in electrophysiology . Next to Long QT, Brugada, DID is looked upon as a new marker for SCD in young as well as elderly .
What is DID ?
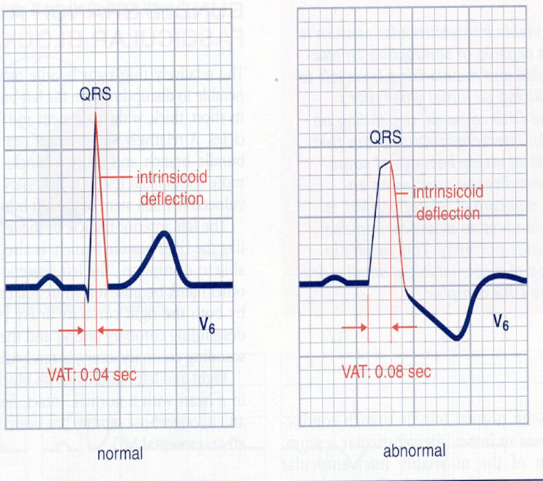
Delayed Intrinsicoid deflection. (DID) Mind you, Intrinsicoid deflection ( ID ) is nearly 100 year old concept, being rediscovered. ID is the time it takes for the electrical impulse to travel from the endocardium to the epicardium directly beneath the recording electrode.
1.How to measure, what is the normal ?
Variable in each lead.
2. Which lead it is measure ? Is ID relevant in Limb leads ?
V5, V6. Normal less than 50 ms
3.When do you call Intrinsicoid deflection as prolonged ?
>50ms
4.What is the Ionic basis of ID ?
Sodium
5.Is there both congenital and acquired forms?
Yes
7.Is it different over RV vs LV ?
Yes
6.How does a DID trigger an arrhythmia ?
Not clear
Two more questions
7.Why it is called Intrinsicoid deflection rather than Intrinsic ?
Intrinsic was the original term coined by Sir Thomas Lewis in 1914, To get this “intrinsic” measurement, an electrode had to be placed in direct contact with the epicardium . Measuring it from surface ECG leds make it Intrinsicoid.
8. Is Intrinsicoid deflection and ventricular activation time (VAT) both are same ?
Yes. Both are used inter changeably , though one denotes time other the wave as such. While VAT is the same time , specifically look at time to R wave peak. However , ID can be applied to the leads where there is no R wave. Then it becomes time to peak of Q
9.Is it true, in every LBBB, ID is prolonged by default ? Then what is the risk of SCD in LBBB ?
For the first part of the question, the answer is Yes. The second part , we don’t know the true risk yet.
10. …………………………………………………………………..(Question left for the readers to ask)
Final message
As cardiologists, we have given disproportionate importance to the QT interval and gets the blame for many SCD. It is time, the 100 year old ECG parameter Intrinsicoid deflection (ID,) seems to be equally important. Much of the secret ionic codes, for many SCDs are believed to hide behind this eerie deflection.
Reference
Here is an important review




{kind=link}