Good bye to Gruentzig … the mercurial genius and the father of Interventional cardiology. The swag attached to PCI has become a bygone era. Percutaneous structural heart disease interventions, though in Infancy, is ruling the world today. Tans catheter heart valves is the new mantra. (THV).We can say Aortic stenosis has been conquered without surgery.(*Note : we means cardiologists, not patients) . Pediatric cardiologists have done the same in percutaneous pulmonary valve delivery in children. However, our quest for percutaneous AV valve implantation is facing tough challenges that sans meaningful outcomes.
It is heartening to witness huge technological innovations in arena of native TMVR*. Still, Mitra clip (TEER ) is the only non surgical solution for MR as of now. We know, It is a terrible alternative for an surgical MVR. The key issue with TMVR is the absence of good native foundation and tackling the extremely dynamic AV ring , which are in continuity with LV/RV muscle (unlike Aortic valve ) Mind you ,the AV valves should withstand the force of TAPSE/MAPSE for tricuspid and mitral valves respectively. May be a dysfunctional left ventricle might co-live with a TMVR with more peace. (Fortunately ,LV dysfunction is common in patients who are considered for TMVR)
*Valve in valve in TMVR is being widely used .The issue discussed here will be for TMVR . native mitral valve diseae.
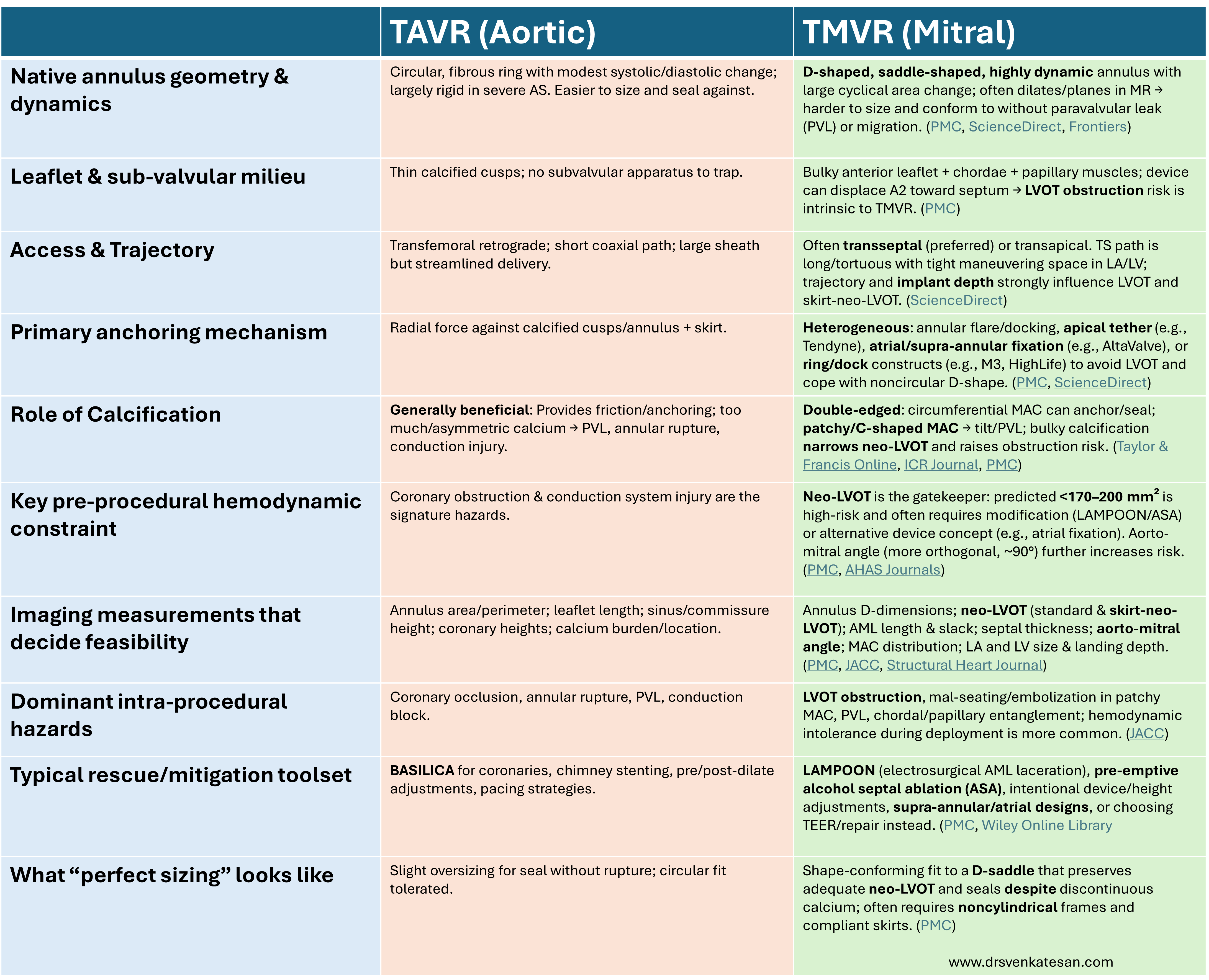
Here , an attempt is made to differentiate the basic differences in the science of between TAVR vs TMVR . (Not comprehensive, but has compared three promising TMVRs , Intrepid, Tendyne, M-3 and Alta-valve.
Final message
Though TAVR and TMVR share a word ‘transcatheter’ they live in different anatomical and physiological worlds. TAVR is often successful because calcium is mostly friendly , the annulus is near circular, and landing zone is fairly predictable. Implantation of TMVR demands extreme diligence because the annulus is dynamic, calcium is an unstable ally, and of course there is always the fearsome LVOT nearby.
Post-amble
Meanwhile, the inability to dispose of the native disease leaflets is a the common issue in both TAVR and TMVR .( which our surgical colleagues will laugh at) May be we need to wait until an new avatar of BASILICA or LAMPOON, which might have a valve bioptome , to cut and extract native leaflet ,safely through a dedicated port without the risk of embolization.



