Does DOACs trying to push over warfarin in post STEMI LV mural thrombus ?
Yes , it seems so. Old must give way for new, even if it is gold. We need to go with the trend. Only thing, we need to prove is, whether the new ones are safe . Need not bother much about efficacy. Some one, will somehow, prove the new ones , non-Inferior to the best available drug as on date.
Every experienced cardiologist would know, Warfarin is many-fold more effective. But, still NOACs are coming in a big way. With the help of big trials, NOACs will ultimately replace the much more dangerous, bleed-prone Warfarin. One more reason we might embrace the inferior drug is the clinical inertia for vigilant INR monitoring.
What does the evidence say ?
Read : Ref 2

The future of medicine will be fight between quality & ( Intention ) of evidence and experience
Caution : Personal opinion
It would be science at its best, when a less potent drug, that requires zero monitoring, will replace a more potent and established OAC. It doesn’t require brilliant brains, to realize a drug which has less bleeding risk, is going to be less effective in getting rid of thrombus as well. (The trial in Ref 2 proved otherwise)
Only issue with warfarin is, we need to be a little more careful. Fortunately, its usage in LV mural thrombi is not likely to be permanent. (as in prosthetic valve)
Reference
AHA comprehensive review on LV thrombus management
A new pre specified -meta-analysis (I don’t know what it means) from a popular Journal EuroIntervention shows a strong evidence in favor for DOACS
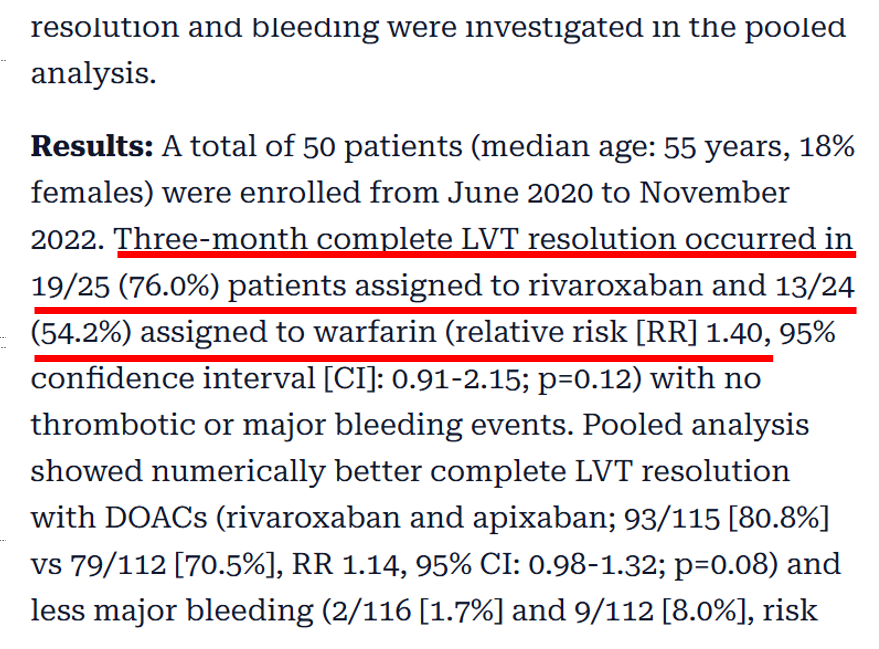
In the above study, Warfarin trails behind Rivaroxaban by a huge 20% margin in it’s ability to successfully remove LV thrombus.
TThere is a surprise in the conclusion : Why do the authors, hesitate to commit DOACS are superior? Something to think about.