Anyone who is flushed with millions can become a member of “The Hurlinghamin” London or the “Yacht” in Monaco, or any other glamorous clubs in the world. But, EBC* is different. Only cardiologists are privileged to enter. EBC is obviously unique. It is the only club addressing exclusively a subset CAD, ie bifurcation coronary lesions. Apart from immense pride and academic entertainment, it teaches us some deep technical points. (By the way, BFL* is a minuscule spoke in the gigantic wheels of global atherosclerosis)
Approach to BFL
90% of BFL still require only drugs or humble single stent or a provisional second stent strategy. However, as per basic rules of human intellect, lesser problems continue to bother us and consume our precise time. This continues, even after realisng , there are 6 complex two stent strategies that doubles up complications.
(*EBC -European Bifurcation club .BFL-Bifurcation lesion)
We will address one unique issue in BFL. May not be a major clinical issue .Still, it’s worth it. It is about the side branch crossing after the intentional jailing of the side branch.
Let us answer this query first
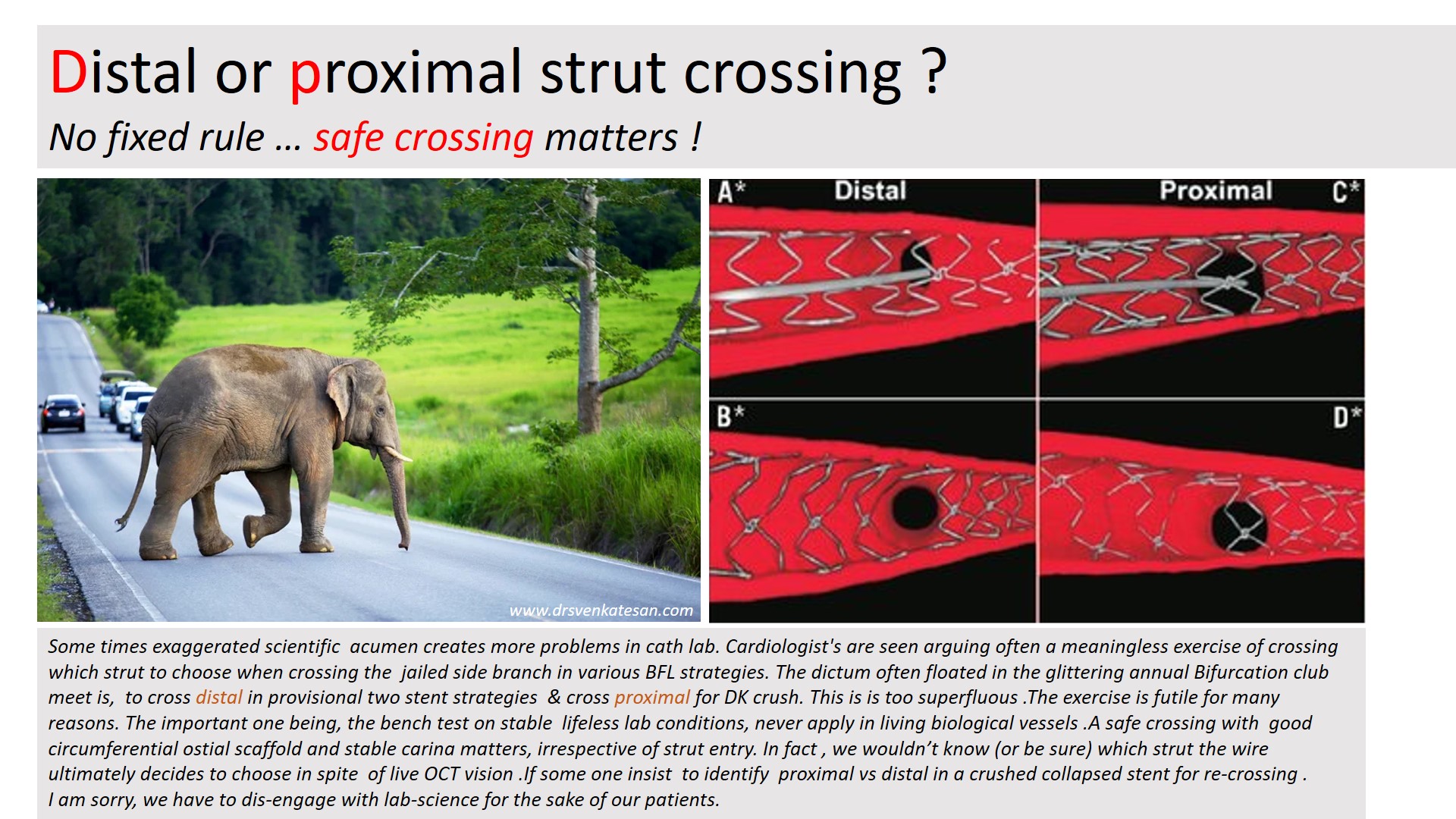
Pure science: Observations from Bench test (Text from Ref 1)
In contrast to provisional stenting in which re-crossing through a distal strut is desirable, initial re-crossing the crushed SB stent in the DK crush technique should be done through a proximal stent strut to minimise the risk of SB stent deformation. A theoretical exception could include bifurcations with a particularly narrow angle for which proximal re-crossing may shift more struts towards the MV, leading to a less desirable, longer neocarina. The 2nd recrossing should be done through a distal strut.
Bench testing is clear. Still , Why this confusion ?
We are all talking about theory in bench testing in stable non-hemodynamic conditions that lacks a biological carina and the dynamics of plaques. We are aware that there are at least 5 virtual ostia in every bifurcation arena (or trifurcation) . The qunatum and direction of plaque sharing occurs with a random effect. We also know the final kissing either cements these plaques perfectly or unsettles in a most bizarre way. So, these strut crossing stuff, are more of an imaginary bio-engineering principles. Whichever strut you cross, do it slowly, gently dilate it to the maximum within the polygonal confluence and good approximation. Don’t get too much carried away , even live online OCT guidance do not guarantee a perfect crossing.
Final message
The answer to the title question seems to be (me), one need not hair-split much on the site of crossing at the side branch. Fortunately, in whatever way, we weave the metallic mesh*, at the epicenter of the coronary highway, it is the natural secretagogues like TPa, Nitric oxide, PGI-2, along with DAPT decides the patient’s genomic fate.
*An appeal to all EBC club members.Before embarking upon a compex PCI on a stable patient , please think for one last time , whether your patient might do well, only with medicines.
Referecne
1.Hall AB, Chavez I, Garcia S, Gössl M, Poulose A, Sorajja P, Wang Y, Louvard Y, Chatzizisis YS, Banerjee S, Xenogiannis I, Burke MN, Brilakis ES; Collaborators. Double kissing crush bifurcation stenting: step-by-step troubleshooting. EuroIntervention. 2021 Jul 20;17(4):e317-e325. doi: 10.4244/EIJ-D-19-00721. PMID: 32310131; PMCID: PMC8919516.



