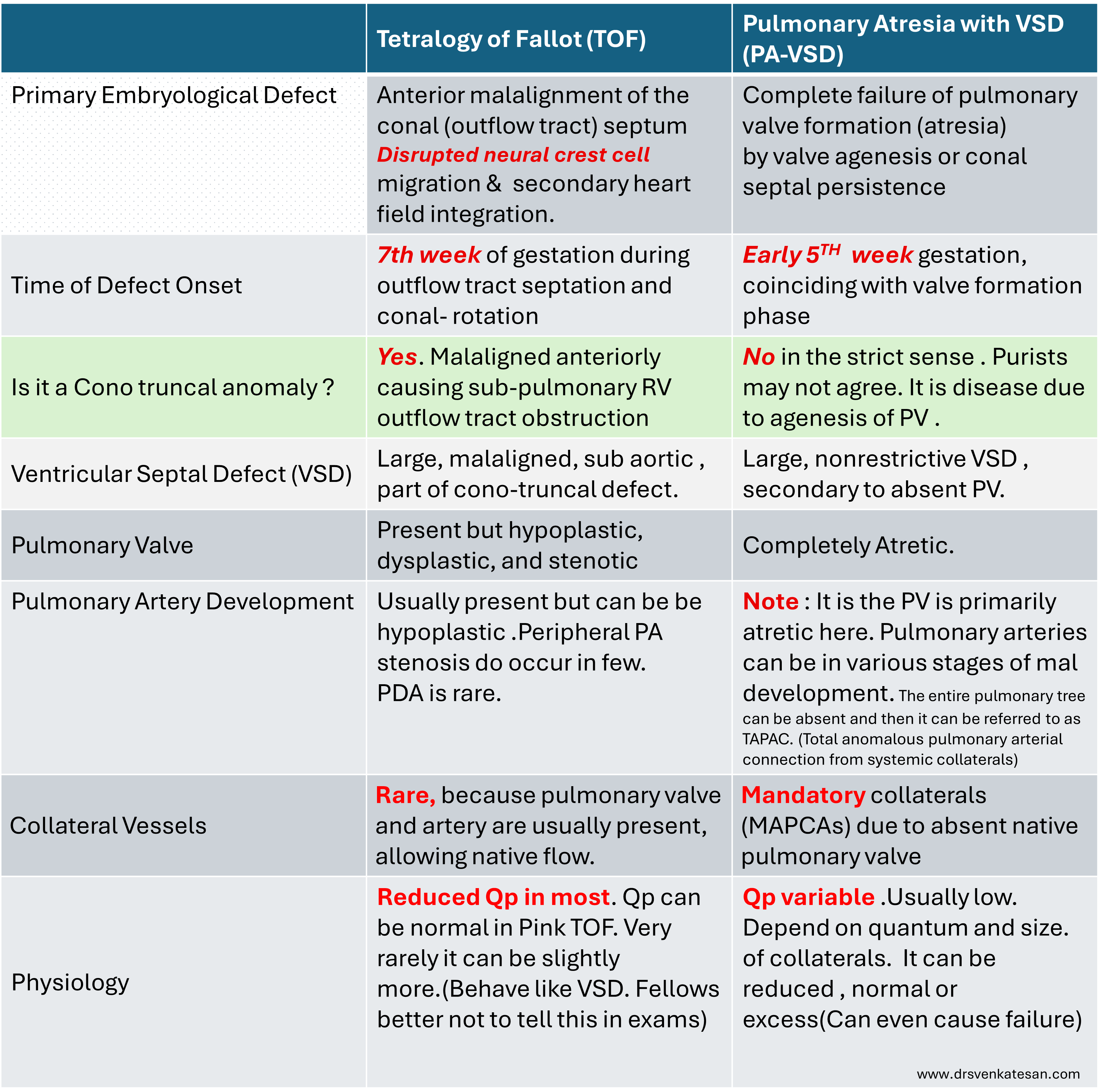
There is a list of conditions that come under cono-truncal anomaly(CTA) in CHD. TOF is the classical example. CTA are group of genetically determined fusion defects between developing right ventricle , septum and the outflows .Many components of outflow are outsourced from cranially located neural crest . In fact, improper migration and fusion of this secondary heart field to the primary is most common cause of many complex heart disease. Microdeletion on chromosome 22, specifically in the 22q11.2 is a major documented gene defect. Traditionally CTA list often includes PA with VSD. This table compares the anatomical and embryological basis of TOF & PA with VSD. You can decide whether to call both as part of cono-truncal anomaly or not.
Add on content.
One important difference is missing in the above table. It is about presence and absence of PDA. In TOF true PDA may be present in early days or months . In PA with VSD , PDA or (MAPCAS mimicking a PDA ) can be part of collateral .A persistent controversy is, how to differentiate a PDA from MAPCAS .That can be challenging. Further, to label a vessel as PDA it should drain into normally formed left pulmonary artery, which is rarely likely.