One of the intensively discussed, but casually taken concepts among the interventional cardiology community is to decide, when to do PCI in a non-culprit vessel in STEMI ? It is more of desire driven, rather than data driven Interventions. ( To fulfill the grandeur- mirage of complete revascularization , which occurs only in lab models )
Evidence pendulum (Ref below : MULTISTARS-BIOVASC-FIRE -COMPLETE–CULPRIT SHOCK)
The pendulum is swinging continuously from immediate multi-vessel PCI to delayed, deferred, (how much or as you like?) The problem is. these pendulums can be set into motion, as we desire , by different stake holders and publish them too in major journals like NEJM, Lancet, etc. The COMPLETE-NESS of evidence is mostly In-complete, if we scrutinse it properly.
Prolonging our playtime in an ACS ridden coronary artery, with a multivessel PCI can be really problematic. Every experienced cardiologist knows this fact. But RCTs (& some peer groups) that come from nowhere confuse them. Of course, some RCTs do give us the right lead. It is very unfortunate that many of us failed to learn an important lesson from the most remarkable trial CULPRIT-SHOCK (Ref 4) that came a few years ago. Since it tried to tie the hands of interventionists, it was not very admired. It proved that, if an ACS patient is hemodynamic shock , don’t touch the non-culprit vessels. (Only a few crazy cardiologists, could extract a vital , but non existent fact from this study. That is, if you want to destabilize a hemodynamically stable ACS/STEMI, try multivessel PCI)
Pros and cons of multivesel PCI in STEMI
Pros are plenty, as we can churn out an RCT as we wish, while the cons are reserved for pessimists, but they are not often imaginary.
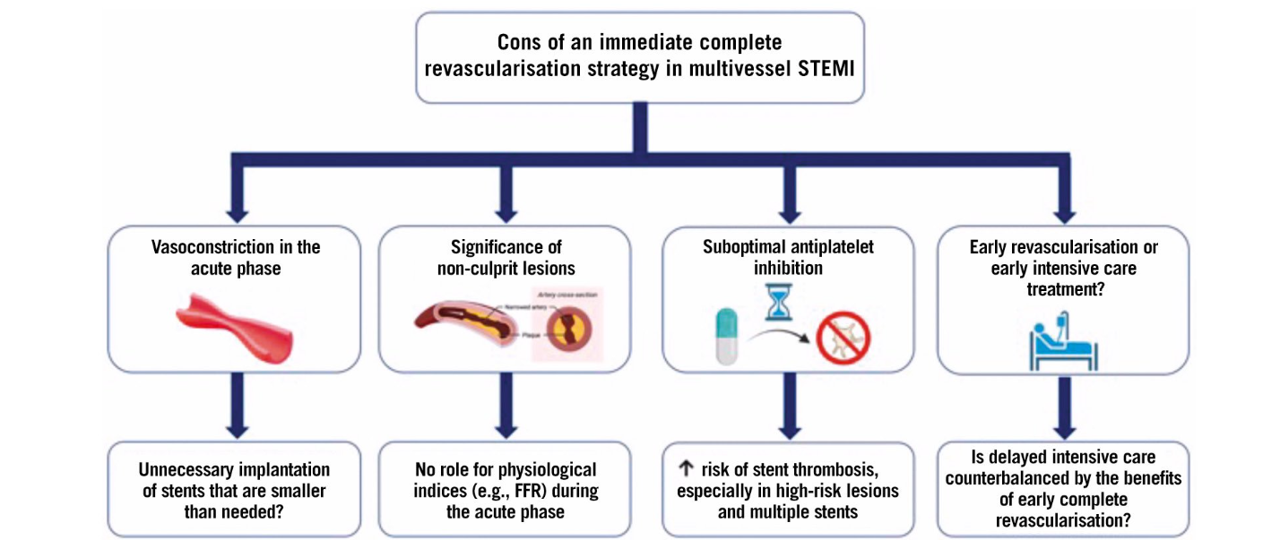
Immediate complete revascularisation after STEMI in patients with multivessel disease carries several important risks. Vasoconstriction during the acute phase may lead to unnecessary implantation of stents that are smaller than needed, potentially compromising long-term vessel patency. The assessment of non-culprit lesions is challenging in the acute setting; there is a distinct vasospastic component amplifying the lesion severity. Further there is no role for physiological indices like FFR to guide treatment, raising the possibility of unnecessary or inappropriate interventions.
Other significant concerns include suboptimal antiplatelet inhibition, which elevates the risk of stent thrombosis, especially in cases with high-risk lesions and multiple stents.
Finally, the decision to pursue early complete revascularization versus prioritizing intensive CCU care can be complex. A cath lab-centric thought process continuously interferes and clouds our intellect and common sense succumbs, i.e., an injured myocardium needs some rest after all, as do a tired cardiologist.
Final message
Should I fix that 80% LCX or 70% PDA in an anterior STEMI?
You are the boss in your lab, what you think must be right, because it is your thought. Also, you are licensed to do whatever you want to do in your patient. But, remember this: These lesions are not real culprits as of now, unless, The RCTs you love instigate them.



