Human body is now approached by many of the physicians as collection of multiple organs . This is the price we pay for modernity in medical science. The era of great physicians in general medicine has gone . Now, a super specialist of one organ is rarely concerned about what is happening to the patient’s other organ , it is considered foreign to him ! While , this is the dominant thinking pattern of modern-day specialist
Let us travel intime and go to the year 1954 . . .
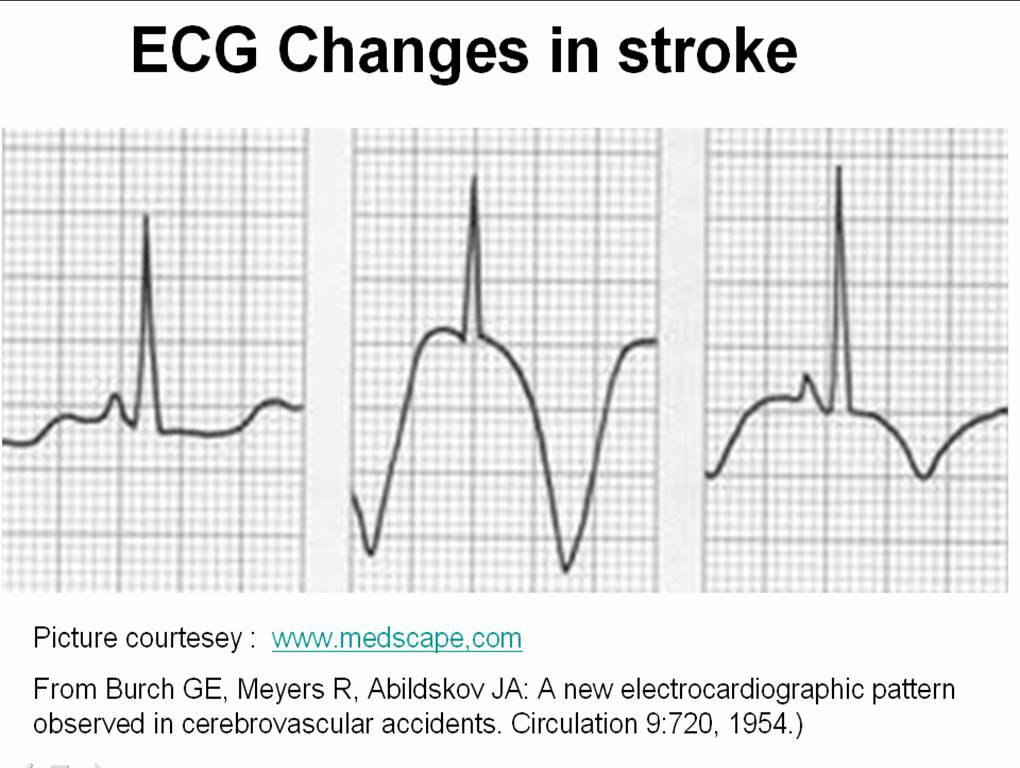
Three physicians from Michigan ,USA published one of greatest observation in clinical sciences , namely the ECG changes in various forms of stroke .
Now , a shrewd physician , will suspect a subarachnoid hemorrhage (SAH) by looking at the ECG when the clinical situation demands . But , what we need is every one should develop that skill . We have seen errors happening even in big institutions (or is it because it is big ?) when an elderly person comes with deep T inversions with or without altered sensorium being rushed into CCUs & cath labs instead of neurology units.
We need to teach our junior colleagues . . . That , ECGs of patients with acute neurological syndromes (ANS) can mimic as acute coronary syndromes (ACS) ( especially in elderly ) .
The following ECG changes * are observed during stroke
- Deep T wave inversion – Sub arachnoid hemorrhage
- Cerebral thrombosis – Prolonged QT interval, U WAVES
- Cerebral hemorrhage – ST segment shifts /T inversion

The ECG changes tend to occur very early after CNS injury.May last up to 1 week. They are not useful to identify the type of stroke. But , deep T wave inversions strongly suggest SAH rather than ICH or thrombotic stroke.
What is the mechanism of these ECG changes ?
It is a clear proof that heart and brain are interconnected by neural network. All the noted changes occur during myocardial repolarisation . (ie ST segment ) The current thinking is (Ofcourse , it is same as our thinking in 1950s !) it is mediated by adreneergic surge initiated by CNS insult transmitted to myocardium by the sympathetic system.
Why should SAH produce more ECG changes than others ?
It is possible the net adrenegic drive from the brainstem and spinal cord will be greater in SAH as it spreads the entire CNS through the cerbro spinal fluid. While localised ICH and infarct is likely to generate less adrenergic impulse.
Reference
Read the link to circulation 1964 .With courtesey to circualtionaha.com
http://circ.ahajournals.org/cgi/reprint/9/5/719.pdf
This came 50 years ago , we still quote their work and no one has improved their work .
Final message
If only we make the clinical bed side teaching as a regualr habit , we do justice to our great physicians of the past , who enriched our life with their clinical skills and passion for knowledge sharing .




{kind=link}
Leave a comment