Femoral artery puncture is still the default technique for cardiac catheterization even as the radial access has gained huge popularity in recent years.Though patient comfort and access site complications are clearly low in radial approach, complex procedures still demand femoral access. The true draw-back of the obsessive adaptation of radial access could be the gradual loss of expertise in the fine art of femoral artery puncture.
It’s true femoral artery puncture can be troublesome at times by palpatory method .How to get into a difficult femoral artery with a poor pulse either due to anatomical reasons, extreme obesity or a compromised hemodynamic status ?
There are times, blind puncture based on anatomical guess could work. Alternate ways do exist. One can access the femoral artery by ultrasound guiding with or without smart needle system . More practical is the empirical puncture based on surface anatomy over the head of femur in fluoroscopic screen.The later method is not really crude as some would think !. It was suggested by Grossman and popularized by none other than father of Interventional radiology Dr Dotter in 1970s .(Radiology Apr;127(1):266-7.Fluoroscopic guidance in femoral artery puncture.)
By fluroscopy , in AP view the head of femur can be divided into 5 zones.(Huggins) Zone 1 and 5 or superior and inferior to head of femur.The zones 2,3,4 are divided into upper, mid and lower third.
Where does common femoral artery bifurcate ?
The bifurcation of the CFA occurred in zones 2, 3, 4 and 5, which was 1%, 9%, 43% and 47% of the time, respectively, and thus occurred within the lower third of the femoral head or below the lower border of the femoral head in 90% of patients.

Image source Cardiovascular Intervention and Therapeutics January 2014, Volume 29, 18-23 Madjid Chinikar
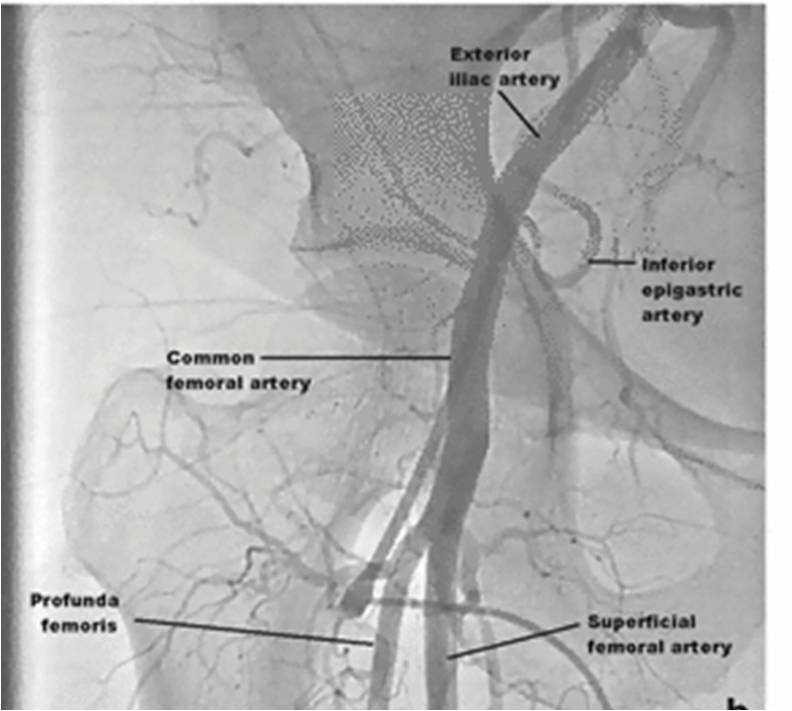
Image source Cardiovascular Intervention and Therapeutics January 2014, Volume 29, 18-23 Madjid Chinikar
How to approach ?
A 18 G needle could be ideal
Puncture the skin at zone 5 inferior border of head of femur. Enter the artery at mid point in the Zone 3.
The chances of hitting the femoral artery is near 95 %
Reference
1.Fluoroscopic localization of the femoral head as a landmark for common femoral artery cannulation. Garrett PD1, Eckart RE, Bauch TD, Catheter Cardiovasc Interv. 2005
Jun;65(2):205-7
2.Fluoroscopy vs. traditional guided femoral arterial access and the use of closure devices: a randomized controlled trial. Abu-Fadel MS1, Sparling JM, Zacharias SJ, Catheter Cardiovasc Interv. 2009 Oct 1;74(4):533-9
3. Fluoroscopy guided vascular access: asking the right question, but getting the wrong answer? Turi ZG. Catheter Cardiovasc Interv. 2009 Oct 1;74(4):540-2



