William Withering the British Botanist of 18th century now laid to rest in the St Barthomlew Churchyard ,Edgbaston is known for his astonishing isolation of the wonder moelcule Digoxin from Foxglove. (Of course, let us not forget original old lady Ms. Hutton from Shropshire who was treating epidemic dropsy with a concoction of herbal Tea ) He reported this in the seminal paper “An account of Foxglove’ in the year 1750 and subsequently became a fellow of Royal college of science.

(The story of Withering and Digoxin is extensively researched and written by Dr Dennis M, Krikler in a classic review article of 1985 JACC )
Near-death experience of Digoxin
After 250 years , saving millions of life, modern science has killed this warrior (inadvertently ?) by a minuscule study with serious flaws called DIG trial *published in NEJM 1997. It exposed the truth that science in flimsy forms can misrepresent fact. Actually many wouldn’t agree its a bad study. But , everyone realised , the conclusion was misinterpreted and disproportionately given weight to one aspect.The conclusion was worded in such a fashion, which sort of implied a negative bias.
*Yes , flaws were discussed in one of our detailed journal club meeting .
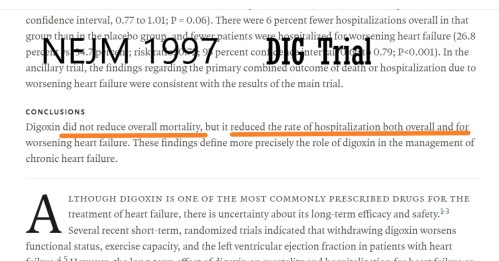
This one study was good enough to smear this drug with a knockout punch as if we are administering poison to a patient with heart failure.Thus a grand old drug became an object of ridicule in academic forums. Subsequent offline real-world scrutiny clearly indicated reduced hospital rate admissions and preventing worsening of HF was directly improving the mortality for which there were no takers. At least occasionally we need to realize there is foolish face for statistics. Now we are beginning to restore some lost sense.
What’s happening in 2019
The same scientific methodology finds Digoxin to have great value . JACC. Awais Malik from Veterans Affairs Medical Center, Washington DC and others try to dig out a truth.
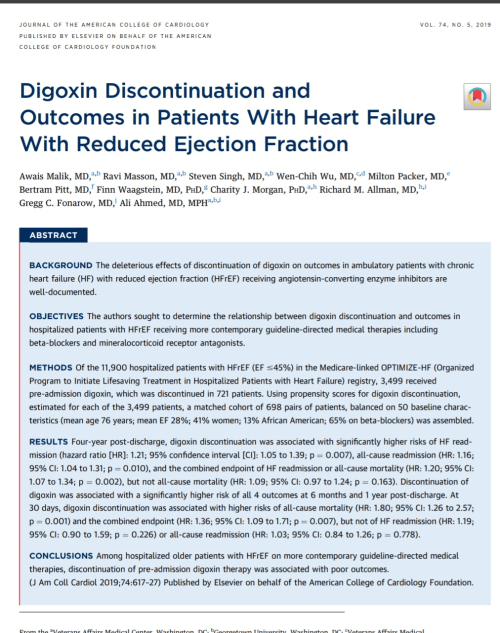
Whoever is blaming this as a withdrawal study are requested to go through the basics of how adding a drug doesn’t help but stopping it worsens. Another group has a different issue. There is a tendency among the scientific community, to look down on studies done in VA hospitals as if they have lesser academic value. I strongly object to that if it’s true. Never have preformed opinion about a study by its source.
How does Digoxin act?
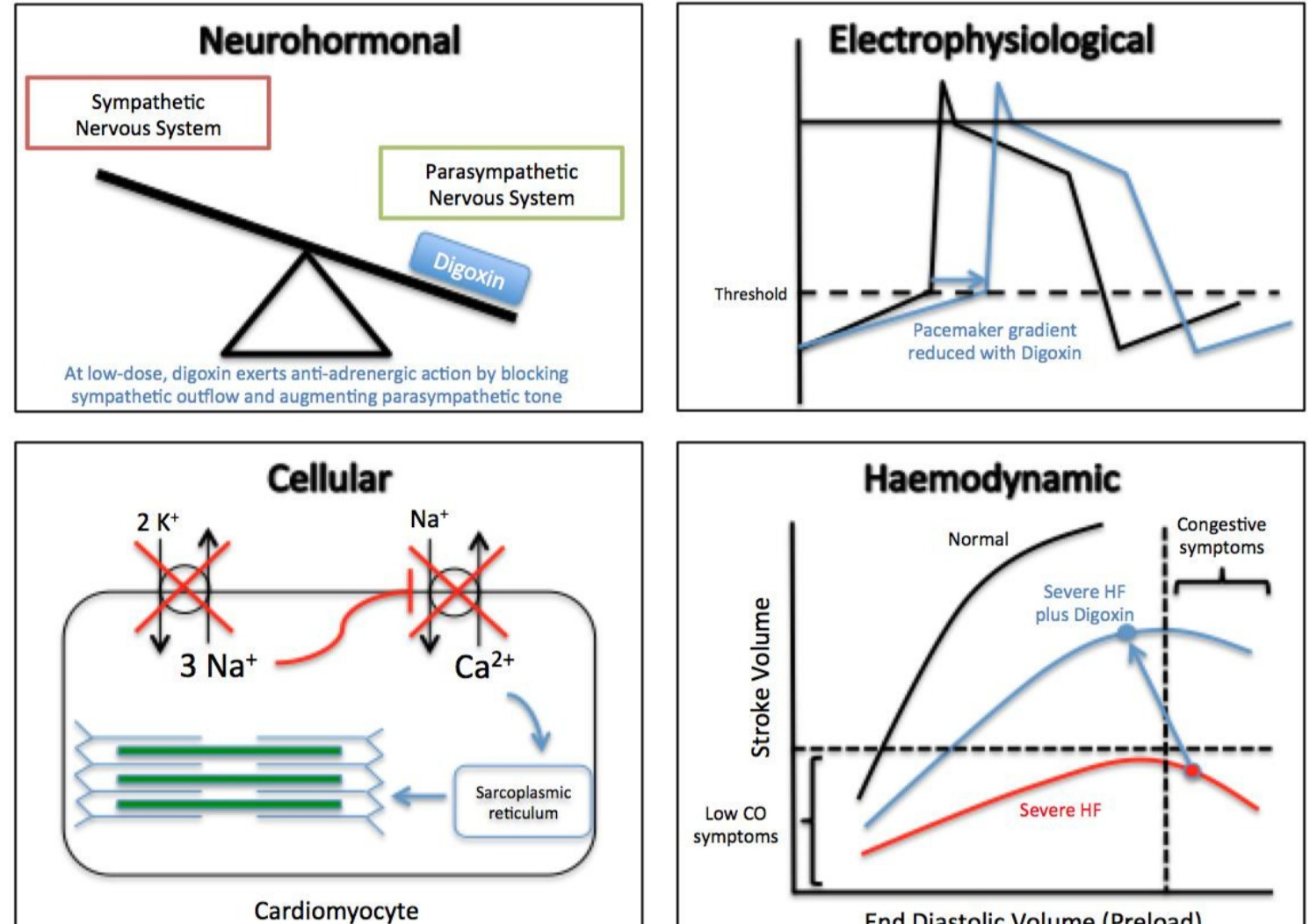
Mind you, Digoxin was working all alone in CHF in the past without the help of all-powerful loop diuretics which was discovered 200 years later, This adds more credit to Digoxin since it has a combined the action of diuretic, anti sympathetic and vagal modulating action, and AV nodal regulation. The only issue with Digoxin could be its safety profile, which if carefully taken care can be overcome. (Afterall, we are trained for this job ) One may call it a most comprehensive drug amongst others in cardiac failure.
Final message
Ignore the greatness of old drugs at your own peril. Foxglove blossoms again, after a gap of 30 years. Please don’t crush it this time! Let Willaim Withering smile from deep inside his resting place at Barthomlew Church along with millions of heart failure patients.
ESC 2020 Update
RATE-AF study reinforces value of Digoxin in AF rate control.
https://www.acc.org/latest-in-cardiology/clinical-trials/2020/08/28/15/59/rate-af

Reference

2.History of William Withering
3.Ahmed A, Rich MW, Love TE, et al. Digoxin and reduction in mortality and hospitalization in heart failure: A comprehensive post hoc analysis of the DIG trial. Eur Heart J. 2006;27(2):178-186
Postamble
A funny business Idea
I guess Parke Davis those days had wholesome rights for Digoxin. May I suggest few tips for the industry how to capitalise this newly generated enthusiasm. Please ensure this drug sounds anything other than Digoxin which seems to have a stigma attached for the modern guys.
Try renaming this drug , a sodium-potassium ATPase blocker, as DiNaKatban and patent it as a unique weekly depot Injection with an attractive 499$ price tag. Another option is to add Digoxin ,Neprilysin and Frusemide, possibly an ARB ( Dinephrimab) and project it as polypill for HFrEF . Publish it in NEJM with a huge non Inferiority trial,break it in ESC or ACC .Consider selling it on all heart failure clinics with a special launch. I am sure, the same guys who ridiculed this drug for so long, will ask their patients to stand first in the queue. Call me, if this new generation Digoxin doesn’t vanish like hot cakes from these pharma malls.



