Sometimes, someone, suddenly asks some silly question. The problem is, we don’t have much of expertise and wisdom to tell whether the question is silly or serious . The so-called sacred ratio of ideal doctor population ratio (1:1000) has come under vigorous scrutiny as the number of observational studies found little relationship between the number of doctors and the health of a society, community, district, or even a country.
This ratio was attributed to WHO, which denies , it had never recommended any such ratio. It only has some suggestions for a combined medical professionals ratio (that includes Doctors, Nurses, and paramedical professionals). We neither have split figures nor its effectiveness.
Here is some new-news in Times of India ,on the topic. It is time for all countries, planning commissions, and health regulatory bodies to do a deep introspection.
Final message
What exactly is the relationship between the doctor-population ratio and the health of a country? May be the toughest question for the entire medical profession. Meanwhile, one of my colleagues wanted to define the number of cardiologists required per unit of population for optimal cardiac care in my state of Tamil Nadu. I told him, let us sort out the basics, then we shall go for the specialist ratio.
A related article and a chat with AI to find an answer to this frivolous question.
This happened some 20 years ago. One of my senior surgical colleague casually asked a Innocuous question to me, when I was in the elevator to reach my ward. “What do you guys really mean by LV dysfunction?” When I looked at him little amused, he said…“I am asking it seriously.” My fellow mumbled to me. that this query is apparently related to the echo report, we gave, few days ago, regarding a patient with AR and severe LV dysfunction .(who is posted for AVR the next week) . I gradually realized the gravity of the situation and question.
The ambiguity is the other name for LV dysfunction
The term LV dysfunction , we use umpteen times a day, simply convey a meaning, that LV is not working well. Is that right? What is it due ? It can be simple wear and tear, fatigue, myocyte damage, ischemic or non-ischemic, myocyte necrosis, death or apoptosis. Beyond that (recall myocytes form only 33% of LV mass, the rest are something else!) Non-myocytic interstitial infiltration, fibrotic, non-fibrotic, scarring, proteo-stasis, neo-cell proliferation, chronic organized myocardial edema. Apart from this, the now outmoded terms like hibernating and stunned myocytes are also included in that LV dysfunction basket.(Finally, don’t forget about hemodynamic afterload mismatch & dysfunctional diastology )
My surgeon friend was right after all. Which LV dysfunction are we talking about? Learned a harsh lesson. Our academic ignorance is explicit, still going around the wards majestically. Realised as a cardiologist we have the responsibility to find , (or at least make an effort) the various components of LV dysfunction.
Mechanism of LV Dysfunction in AS vs AR
Differences in Mechanism
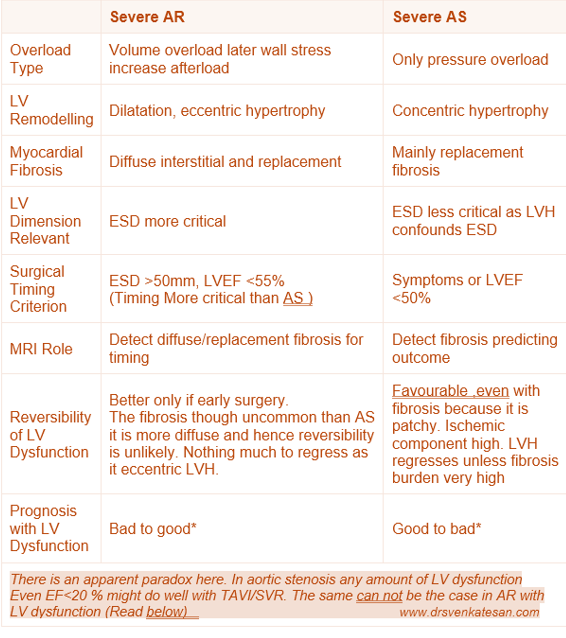
AR involves volume overload with LV dilation and eccentric hypertrophy with diffuse myocardial fibrosis. AS involves pressure overload with concentric hypertrophy and more focal replacement fibrosis. Both conditions lead to fibrosis, but the pattern, timing, and extent vary.
Clinical Implications in Timing of Surgery
Surgery in severe AR should be considered before irreversible LV dysfunction, guided by indexed LV dimensions (especially end-systolic diameter >50 mm or indexed >25 mm/m²), or LVEF <55%. Waiting too long allows fibrosis and remodeling to reduce recovery chances. In severe AS, surgery is indicated once symptoms develop or LV ejection fraction falls below 50%.
Role of LV Dimensions EDD and ESD
LV End-Diastolic Diameter (EDD): Reflects volume status and remodeling, important for AR where volume overload is predominant.It is less useful as it is pre-load dependent.
LV End-Systolic Diameter (ESD): ESD is unique parameter as it represent a topmost point ( north west) in cardiac pressure volume loop , when the contractility is load independent . it is a strong predictor of contractile function and prognosis.
Role of Cardiac MRI in Identifying Reversible LV Dysfunction
Role of MRI is vital. Cardiac MRI uses late gadolinium enhancement (LGE) to detect replacement fibrosis (scar) and T1 mapping/extracellular volume (ECV) quantification to detect diffuse interstitial fibrosis. *LGE: Late mean 20 minutes , the tissue stagnates and fails to get wash off and appear enhanced
Reversibility of LV Dysfunction in AS & AR : Is there a paradox ?
Patients with severe AR generally exhibit better reversibility and prognosis post-surgery compared to those with AS, (Ref 7 : This study found patients AR tend to have more diffuse fibrosis, which exhibits better regression after valve surgery compared to the focal replacement fibrosis in pressure overload conditions (like AS). This suggests better reversibility of LV dysfunction in AR) This finding is an apparent paradox, since we think LVH is more likely to have fibrosis.
Timing of surgery is more critical in AS or AR ?
Patients with severe AS and very low LVEF can still experience significant improvement in LV function and survival after AVR.
The explanation is that in AS, the primary problem is a mechanical pressure overload due to valve obstruction. AVR abruptly relieves the afterload, decreasing LV wall stress, and allowing recovery of myocardial function, sometimes dramatically.
Even patients with severely reduced systolic function can see meaningful functional recovery post-AVR if myocardial fibrosis and irreversible damage are not advanced.
AR Patients with Moderate or Low EF After AVR
In contrast, patients with AR who have even moderate reductions in LVEF tend to have worse outcomes post-surgery.
The explanation lies in the gradual volume overload and progressive LV dilation in AR, leading to more diffuse myocardial remodeling and fibrosis that may be less reversible.
The reduction in afterload after surgery in AR is more gradual and less dramatic than in AS, and by the time EF is moderately reduced, irreversible myocardial damage often limits recovery.
Thus, surgery is ideally timed much earlier in AR (before moderate EF decline) to optimize
The non-forbidden question
Why should we wait? Is time a muscle only in ACS? Not in valvular heart disease? Can’t we intervene in all patients with severe AS/AR irrespective of LV function before it worsens?
Yes, time is indeed muscle even in VHD. This concept looks attractive. Many centers follow this, ignoring the current guidelines. (The issue here is dependence on artificial valves for the rest of life and the attendant risks.)
Final message
It is indeed true, cardiologists use the term LV dysfunction so commonly and casually, without elaborating on its true meaning. Whenever and wherever possible, we must take efforts to list and quantify various components of LV dysfunction, and also the likelihood of reversibility.
During pregnancy, there is upto 50% rise in blood volume, 70% cardiac output and 20% elevation in heart rate. All of which , will surely hike the transmitral flow and gradient . The transmitral gradient in patients with moderate mitral stenosis ( mitral valve area of 1.0–1.5 cm² ) has a baseline gradient of 5–10 mmHg at rest .It can increase by 2–3 times compared to pre-pregnancy levels. Though exact amounts vary by individual factors such as baseline severity, heart rate control, and overall cardiac reserve.According to the Gorlin formula, the transmitral pressure gradient rises approximately with the square of the increase in flow rate, leading to elevated left atrial pressure.
Mild MS can elevate from 4 to 12 mmHg. In moderate cases, it can hike from 10 to up to 30 mmHg. Clinically, symptoms often worsen by one New York Heart Association (NYHA) functional class. Echocardiography may overestimate severity due to the hyperdynamic state. Some times ,it is very possible , a modertate MS is pushed into severe .Here ,we need to focus on valve area rather than gradient alone for assessment. Labor further exacerbates this, and post-delivery, one can expect acute pulmonary congestion with a fair degree of certainty. Prophylactic diuretics have mitigated this. Paradoxically, excessive blood loss might comfort these heart, due to less preload provided they are not otherwise hypoxic or anemic.
Can we predict who will tolerate Labor
Yes, predciting the course during labor (e.g., decompensation leading to pulmonary edema, arrhythmias, or need for urgent intervention) is difficult but we have some validated risk stratification tools studies like the CARPREG (Cardiac Disease in Pregnancy) risk index. In reality,these scores are practically useless in bed side. All we require is an answer to this question. Will she or (won’t she) need a urgent PTMC or not ? Again a caveat . If significant MR or claciifcation is associated , this question becomes null and void.
Management
It is done in specialized centers or dedicated cardio obstetric units. Involve beta-blockers , many of them are in AF , rate must be controlled, diuretics for volume overload, some of them need antocoagualnts and should follow the standard protocol . Planned PTMC is considered for symptomatic moderate cases during pregnancy if medical therapy fails. ( Ideal to do PTMC in preconception stage ) Doing a elective PTMC in stable patients is a tricky decision especially if they have crossed the first hemodynamic stress zone of 20-24 weeks. There after nothing much to gain in terms of hemodynamics. Of course, the second danger zone of peri labor period is the issue be tackled .
The unexpected good news
Though all the risk predicting tools portray a dismal outcome in moderate and severe mitral stenosis, real world scenario appears better. In this analysis from Rhode Island, USA, which analyzed the data from two other studies from Silversides and Hammed, showed zero maternal mortality and stroke. The only thing observed in severe MS was that all required admission.
Pulmonary edema was seen in 20% of mild stenosis , while it was around 40% in moderate and 60% in severe. The positive aspect about this complication is , all these apparently serious episodes were managed by drugs with thumping success. This implies, the mandatory or enforced PTMC in moderate to severe MS during late pregnancy is largely not necessary. The risk of the procedure to be weighed against the competence of medical management during labor.
Predicting the likelihood of acute elevation of trans-mitral gradient and pulmonary edema is a huge medical guess game . A multitude of factors play a role. Ofcoourse , It elevates in all. But, the consequence vary between innocuous to near fatal.The message from the above study is, since the complications are anticipated, a pulmonary edema is often well managed medically or can be prevented with vigilant monitoring.
Final mesage
Many cardiologist might feel it is scientific to watch a young women with significant MS lying quietly looking ahead a uncertain labor. This is more of our respect to science than the true hemodynamic reserves these women have*. If the facility and expertise to do PTMC is readily available, well and good. If it is not, need not feel guilty and panicky . Track record reveals even severe MS rarely leads to a catastrophe. Thanks to the dramatic resilience of our young pregnant women with an agile cardiac and vascular reserve and also the advanced cardio vascular support drugs and gadgets.
*Legal postures and academic guidelines are rarely in sync with reality of experience
1. How is that ? Cardiac contractile function is normal or even supernormal, in spite of total myocardial disarray and haphazard architecture of sarcomeres?
The simple answer is we don’t know. But the same contractile units, while hyperfunctioning during contraction are not in the same mood of normality and struggle to relax . LV relaxation defects are always subnormal. Let us hope Mavacamten and its siblings could do something about it, converting HCM into from a super-inotropic state and into super- lusio-toropic state.
2. When does genotypic risk profiling more important before phenotypic risk in HCM ?
After decades of molecular research, 1500 mutations in over a dozen contractile filaments, we are in a total molecular mess, regarding which mutation is more arrhythmogenic and which can result in rapid progression of LV mass and fibrotic processes. As of now, phenotypic expression is considered more predictive, except in families with strong family history of multiple sudden deaths in young age. Though the guidelines are too tentative , for sacred scientists, HCM specific genetic profile testing are widely available for both use and misuse.
3. Does relieving LV outflow obstruction improve diastolic function with myectomy /septal reduction surgery?
Yes, it does in many cases, not in all obviously. Can we predict it before the procedure who are likely to improve their diastolic function ? . We can’t, we can only hope. The relationship between LVOT obstruction and diastolic filling is minimally related and curiously unpredictable. HOCM is a universal myocardial disorder .Logically, it is too ambitious to expect, getting rid of few grams (typically 5-15grams) in LVOT area to improve the LV inflow stiffness.
However ,many times , the improvement in diastolic function depends upon the surgical technique .Simple removal few grams of septal myocardium doesn’t guarantee a reduction in overall improvement of diastolic dysfunction. The chordal alignment, mitral cup reconstruction, and restoration of geometry of the LV are all important.
4. Is it true that the risk of SCD is almost the same for Obstructive and Non-obstructive HCM?
It appears to be true. Available evidence are as usually conflicting. Currently, the risk seems to be same or slightly higher with HOCM. Some studies telling us, overall SCD risk in all HCMs are equal .(this may be skewed, because HCM outnumber HOCM )
Further, the dynamism of obstruction prevents us from understanding the contribution of other obstructive elements. Also acute hemodynamic triggers can instantly convert a simple HCM to severally obstructive HCM, hiking the intracavitary pressure and eliciting an arrhythmia and possible SCD. If we realize. the primary underlying mechanism of SCD is fibrotic arrhythmogenic focus , we can guess , how narrow the true risks between these HCM & HOCM .
This chart is gathered with pooled data . The learning point is 10 year survival is dramatically lower in HCM the annual mortality and SCD risk in HCM is not that much comforting when compared to HOCM. I think, the data is still less enough to conclude on the risk of SCD.
Type of HCM
Annual Mortality (%)
10-Year Survival (%)
SCD Annual rate (%)
Overall HCM
1.1–1.3%
65–80%
0.3–0.7%
Non-obstructive HCM
1.1–1.5%
97%
Slightly Lower* or Equal ** or even higher***(Ref 2)
Greetings from Chennai. It all started with some flashy classroom scribblings in Madras Medical College in the year 2008. I never imagined it would reach nearly two decades of writing. It has since reached 6 million visits in 180 countries. My thanks to all those readers and followers for making this possible. As per the request of many of you, it’s been converted to eBook format on Amazon Kindle. It is arranged in a yearly fashion .Currently published as Volume 1 . It will be live document and continuously updated.
Each and every article of the past and the future will continue to be open source on this site. Again, I shall reiterate , the book format is published only to facilitate learning in a single book format and with near- zero commercial Intent. If I do, it will be against the core concept and ethics of this academic endeavor. Of course, whatever little readers think they can contribute by buying this E-book, it will help sustain this site. Sharing the link to the book. I think as of now it is live only in India. Soon it will be globally available. https://amzn.in/d/euhL5vu
What is the mechanism of exertional dyspnea in HOCM?
Is it the obstruction or the restrictive diastolic function? It is easier to say both are equally responsible. Of course, that could be the correct answer, but a true academician need to go further. Among the two ,which is the dominant mechanism ?
As we are wondering what exactly causes dyspnea in HOCM … If we think for a minute, a simple fact seems to clarify everything. Try answering this question. Is dyspnea more common in obstructive HCM or non-obstructive HCM? The answer is not an unequivocal yes .There is definitely no linear correlation between dyspnea and degree of obstruction. This clearly tells us obstruction is not the primary culprit. We got the answer already. (Ref 3)
Other mechanisms: Dyspnea due to reduced forward output is rarely an issue. Associated MR can be a significant factor as MR – v wave pulses can directly trigger the pulmonary venous receptors. High intraventricular pressure stretching the LV mechanoceptors is also a reason. (Its more important in syncope though) In elderly, associated ischemia and CAD can contribute to dyspnea.
Clinical implication of this question
HOCM is a mystery genetic disease, with total myocardial disarray. Still, patients are blessed with hyper-contractile ventricles. No one understands how this is possible. What we need to do is pacify these aggressive contractions. That’s why beta blockers and calcium blockers have been used for decades. Now Mavacamten is introduced to correct the basic defect.
Mavacamten is a new class of drug that targets and corrects the underlying molecular defects of HCM .It is a Selective cardiac myosin inhibition , Reduces active myosin heads by reducing the number of myosin heads that can enter the active, force-generating state. Mavacamten stabilizes myosin in an inactive, energy-sparing conformation known as the “super-relaxed state.” This results in decreases contractility . Relieves LVOT obstruction and indirectley improves diastolic fucntion. lower filling pressures.
Is Mavamten really worthy ? What is the indication ?
Basically, it is a negative inotropic agent. Mind you, beta blockers are a great class of Nobel Prize-winning wonder drugs for this purpose. Calcium blockers too play an important role. But,we are living in a new age, a new era. We have to move on in life, hence we are forced to switch to different agents whether we like it or not, whether it works or not.
What does the evidence say?
Mavacamten is proven to be useful in HOCM in the VALOR-HCM trial published in JACC 2022. Though the MAVERICK trial showed some promise in non-obstructive HCM, the recent 2025 [ODYSSEY-HCM trial](DOI: 10.1056/NEJMoa2505927) did not provide any positive benefits.
Final message
Every patient of HOCM turns out to be clinically, and hemodynamically a full-blown HFpEF and even technically an RCM-plus. In this context, drug research must be directed at more positive lusiotropic agents (Than negative Inotropics) and anti-fibrotic drugs.
Coming to the title question, if I can manipulate the cardiology linguistics , it can be concluded like this. In HCM/HOCM, the primary symptom is diastolic dyspnea due to restriction and the systolic dyspnea due LVOT obstruction contributes a lesser degree. ( Then why all this Septal reduction stuff ? Please don’t ask this question)
AI is now more than a buzzword. Though, it is a creation by modern humans , It has become omnipresent and omnipotent . We realize ,the impact of AI in medical profession is going to be tremendous.
Here is an MCQ on the future of AI in Medical practice . There are two components to it. You need to choose two answers. Both can be the same or different.
1.Which of the following, is most likely to be the dominant theme in the future of AI ?
2.Which one is best for our patients ?
A.Artificially Intelligent machines
B. Artificially humanised machines
C. Artificially Ignorant machines
D. Naturally Intelligent machines
E. Naturally Intelligent humans
Answer:
I know, obviously the responses are too crazy…some of you, might leave this page by now.
But, one thing is very certain, what is going to be the dominant theme & what is best for the patients, can never be the same.
Post-amble
Q 1 .In my view, the current trajectory of AI, will take the future to response C (or B, if god willing)
Q-2. Fortunately, there is no ambiguity here.What is best and desirable for mankind is response E . (But, with an important caveat. Intelligence per-se, plays little role in medical profession, unless it is accompanied by character ,compassion ,honesty and empathy )
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.