Nearly a century ago, Carl Wiggers helped us understand the dynamics of cardiac cycle with a historical diagram depicting systole and diastole. We know diastole has 4 phases. They are IVRT(nil) early rapid filling,(70%) diastasis,(0-5%) atrial contraction(25%) (Percentage filling within the brackets)
What is mid diastole?
The easiest way to define mid diastole is to divide diastole into three parts with reference to time and call the mid-third as mid-diastole. (.5 seconds/ divided by 3). But, Physiologically we can’t do that. Even hemodynamically there is no distinct mid diastole as diastole is divided into 4 phases as described earlier. When there are 4 parts how can we slice out mid diastole without an overlap?
So, what shall we do? Technically which is the best period to be referred to as mid diastole?
Maybe diastasis. In this period either little or no flow occurs. HR heavily influence the duration of diastasis. Cardiologists especially during auscultation created the concept of calling anything happening after mitral valve opening as mid diastole. ie after IVRT which equals* A2-MV opening interval (In the true sense, it must be the early diastole that can begin with mitral valve opening for physiologists, but for cardiologists, it begins with aortic valve closure because we can hear only closing sounds)
What happens in mitral stenosis?
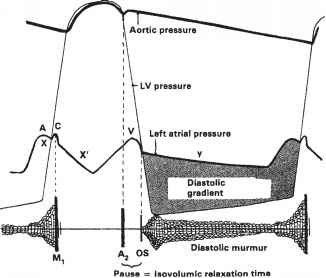
Any significant obstruction of the mitral valve, the gradient builds up immediately after the mitral valve opens. The murmur gains momentum in the early rapid filling phase of diastole, gradient spills over to fill the diastasis, and finally accelerates in pre-systole to end up in loud S 1.
Is there really an early diastolic murmur in mitral stenosis?
(I can’t agree. We were never taught that way)
Yes for sure. In fact, it can be the dominant murmur in many, since the early rapid filling phase of diastole contributes 70% of filling. In mitral stenosis, the early diastolic gradient will always be present. So. mitral stenosis murmur indeed begins in early diastole and extends further depending upon the severity.
If there is really an EDM in mitral stenosis, why do we still keep calling it MDM?
Just by tradition and for convenience. Auscultatory mid-diastole is different from hemodynamic mid diastole. This irony occurs because murmur descriptions are based not on time but on phases. So, by convention, a murmur that does not occupy the IVRT phase is labeled as MDM. This also helps us to differentiate MDM of mitral stenosis from aortic regurgitation which has the exclusive rights to be called an early diastolic murmur.(Since it occupies the IVRT phase)
Final message
This is probably a too-long post to unmask a trivial nomenclature issue in the diastolic murmur of mitral stenosis. Still, it’s worthwhile to understand this. The word “mid in MDM” is arbitrarily used and doesn’t really reflect either the time or the true hemodynamics. In fact, the same reasoning is applicable for any flow murmur across the mitral valve that is inappropriately referred to as MDM.
Caution
*Let me not confuse the youngsters especially undergraduates. MDM of mitral stenosis will remain as MDM in exam halls. It will never become EDM as that of AR where the murmur starts in the IVRT phase.
For advanced readers
What is the earliest murmur to appear in mitral stenosis?
The first noise comes in the early part of diastole or late presystolic when atria contracts. Never in true mid diastole and gets filled up the in mid part as the disease progresses. So, we can have mitral stenosis without murmur in mid diastole. The morphology of murmur can best be understood when we correlate with Doppler echo profiles.
Is MDM of mitral stenosis crescendo or decresedo or both ?
Normally in diastole crescendo murmurs are uncommon as pressures are falling.( Ventricular contraction only can generate crescendo pressures.) Still, In mitral stenosis, there is minimal crescendo at the onset even when the E velocity decelerates. However, there is a definite presystolic accentuation with atrial contraction which can also be referred to as late diastolic crescendo.
*Is IVRT the same as the A2-OS interval?
It is almost the same but not the same. Find out the difference.
Further reading