This is a very crucial question debated, by cardiologists , cardiac surgeons for long decades (of course our patients too need an answer desperately)
Will CABG prevent or reduce future MI risk ?
The answer is not at all simple , most of us are still tentative.
Have a look at the conclusion of these two famous studies. STICH and STICHES. Hope, we could reach closer to a clear answer.Ofcourse, the study population may not fit in to all the CAD population we come across. Still, it conveys some useful information about this issue.
Final mesage
It is indeed true a STICH in time , really saves nine.
Postamble
The toughness of answering this question lies in the fact, it takes hardly three minutes , for a non flow limiting 30% lesion to transform to a life threatening ACS.
Real world data reveals, most patients with multivessel CAD harbor, a minimum of half a dozen non flow limiting lesions. CABG has a huge edge, in this situation ,as most of these lesions are proximal to bypass conduit.
Counter point
Lastly , and most importantly, it is the intensive medical management and life style modifications, that will determine, whether CABGs are going to work, as it did , to the lucky patients of STICHES cohort.
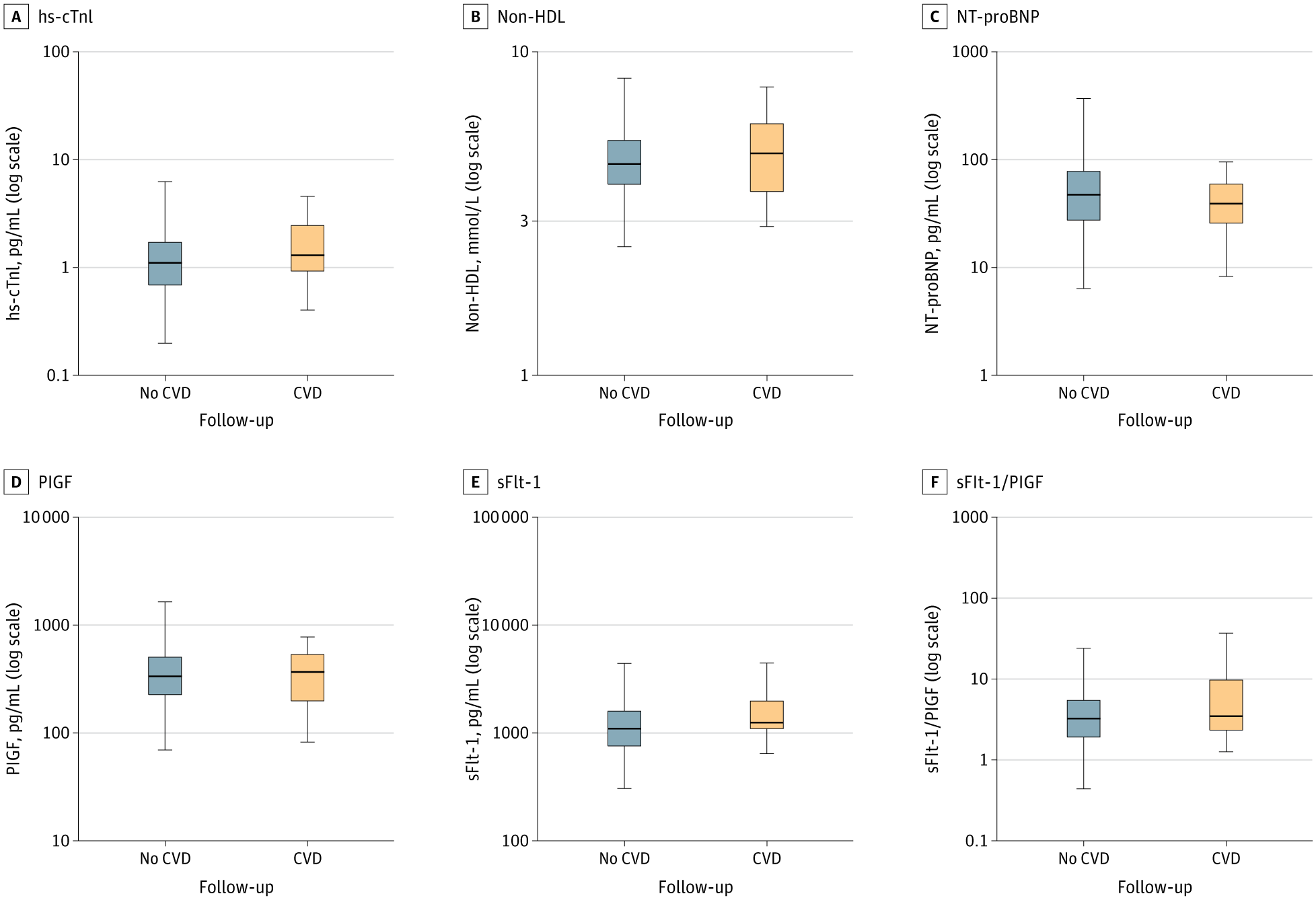
The study in recent issue of JAMA Cardiology examines clinical factors and biomarkers (likely NT-proBNP, troponins, SfLT, lipids) measured during pregnancy to predict long-term maternal cardiovascular disease (CVD) risk, positioning pregnancy as a “stress test” window. Its strengths include a large cohort, long-term follow-up, and subgroup consistency, offering actionable early risk stratification to guide preventive interventions and improve outcomes in women
Design Flaws
This cohort analysis reports CVD prediction over a median follow-up ( 10+ years). The major problem with this study is , it has omitted several key confounders that could bias long-term CVD predictions from pregnancy biomarkers, including pre-pregnancy BMI/obesity, smoking status, family history of CVD, socioeconomic status, psychosocial stress/depression, air pollution exposure (e.g., PM2.5), genetic/epigenetic factors (e.g., polygenic risk scores), These time-varying elements, unadjusted in Cox models, likely inflate biomarker associations over the long follow-up period .
Boxplots show the distribution of biomarker concentrations, stratified by the occurrence of CVD during follow-up at gestational up to 29 weeks. hs-cTnI indicates high-sensitivity cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide; PlGF, placental growth factor; sFlt-1, soluble fms-like tyrosine kinase-1; HDL, high-density lipoprotein cholesterol.
Final message
It is well known that pregnancies complicated by HT and GDM may add future risk for CVD. Using pregnancy as a universal cardiovascular stress test may appear good on paper …but it can’t be purely biochemical prediction. It should be primarily clinical follow-up and accounting for other influential risk factors. This study is too much extrapolated and biochemistry focused. Suggesting a costly biochemical panel to predict CVD risk in a huge population of pregnant women appears a futile extravaganza.
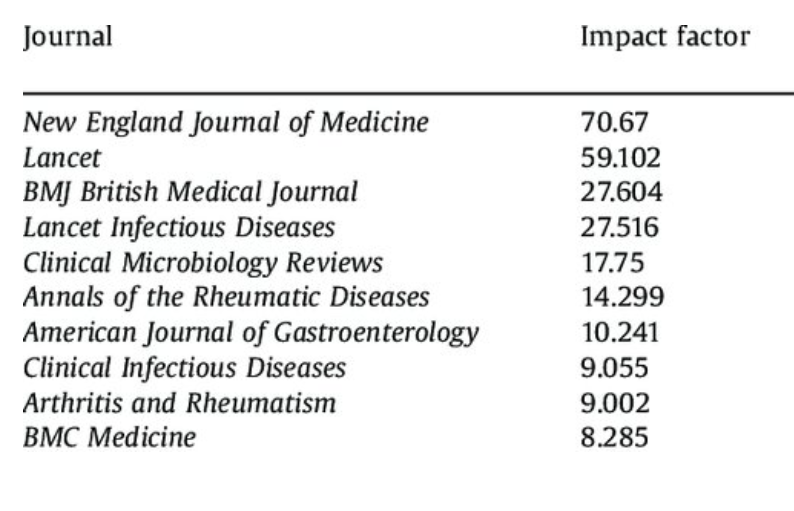
The perceived superiority of journal impact factors (IF) creates a false hierarchy in academia, often equating high IF with superior research quality despite its flaws. Now true scientists are thinking how to counter this hype by advocating for assessments based on actual content and contributions, marking a vital shift toward fairer evaluations.
Pseudo-Superiority of IF
IF confuses journal prestige with individual article merit, as a few highly cited papers skew averages while most receive minimal attention . It fosters misuse in promotions and funding, and invites manipulation like self-citations or favoring reviews . Most importantly, ignores experince and locally published science . The current research assessment models falsifies innovation, ethically burdens top journals, and penalizes genuine works that lacks immediate citations .
DORA’s Welcome Role
DORA explicitly urges eliminating IF reliance for evaluations, prioritizing scientific content, diverse outputs (e.g., datasets), and qualitative metrics With over 2,500 signatories, it drives cultural change in academia, including medicine, by promoting article-level assessments and reducing IF hype .This movement fosters equitable progress, allowing evidence-based research to thrive beyond journal names .
Final message
In this AI era , very often IF also makes an artifitical Impact in academia. Believing IF, as an index of greatness of a research paper … can be a sign of scientific illiteracy. Let us become a member of DORA and try to catch up with the pathways to truth.
From kindergarten, we cherish stories. After adolescence, we dive into fiction. Then in college , science becomes sacred , and we believe, it is an eternal truth.
What a naive notion ? Science mirrors fiction and evolves relentlessly. Yesterday’s facts, become today’s fallacies with the stroke of a keyboard.
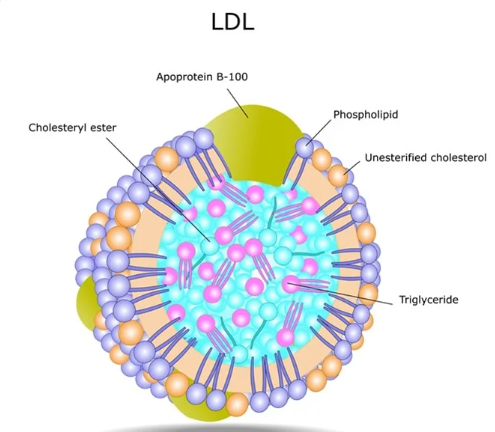
The myth of HDL as “good cholesterol” has been continuously propagated to the public and is etched in our (Patients & Physicians) minds. Likewise, LDL’s portrayal as the ultimate villain persists. Yet, emerging evidence flip-flops this narrative. Large, buoyant LDL particles appear harmless, even protective, while dysfunctional HDL may harbor hidden dangers.
This ignorance-based lipidology stems from oversimplified dogma, that ignores particle size, protien content, and its function. Large, fluffy LDL evades arterial infiltration, unlike small, dense variants. Meanwhile , dysfunctional HDL, oxidized or inflamed, loses its anti-atherogenic prowess and may promote oxidation and inflammation. (This may look like an exaggerated statement, but the fact that the largest popualtion at CAD risk : south asian metabolic syndrome, have a normal LDL level , tells us a chilling truth and mis- understanding about the lipid mediated CVD.
The curious paradox in dyslipdemia : It is the protien fraction that dictates the risk & benefit
In dyslipidemia, a key paradox exists. The protein fraction apolipoprotein that determine true risk and benefit, not lipid content alone.
ApoB-100
Apo B100 forms the structural backbone of atherogenic LDL. There is one Apo B 100 particles one molecule of LDL. It quantifies total harmful burden.Unlike LDL-C (which measures cholesterol load), ApoB-100 directly tallies particle count for superior CVD risk prediction. In large buoyant LDL, reduced ApoB-100 atherogenicity makes these particles largely benign and non-infiltrative.
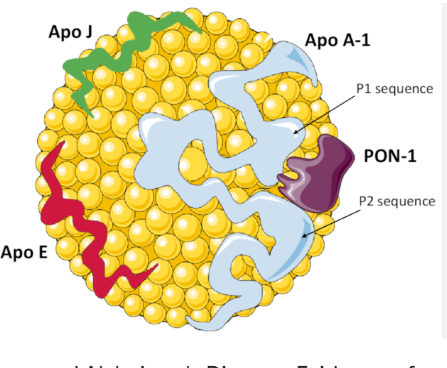
ApoA-I/ApoA-II in HDL
ApoA-I (70% HDL protein) activates LCAT for cholesterol esterification and drives ABCA1-mediated efflux from macrophages. It also suppresses LDL oxidation and vascular inflammation, embodying HDL’s core anti-atherogenic shield.
HDL structure
ApoA-II stabilizes HDL size/composition but impairs ApoA-I function in dysfunctional states converint HDLto a pro-inflammatory molecule. ApoB/ApoA-I ratio is key for the proper functioning of HDL. It is also proven, that the beneficial effect of HDL is lost beyond 60mg/dl.
Final message
Whenever we discuss hyperlipidemia, we falsely blame the lipids for endothelial injury .Realistically ,it is the protein sub-fragment Apo B 100 , which acts like a knife and hides within the lipid core , and attack the intact endothelium. There is no empty or toothless LDL molecule without Apo-B. However, there is a well known phenomenon of large bloated LDL , with excess foamy cholesterol,that sort of covers sharp edges of the Apo-B* like an umbrella and reduce the risk of endothelial injury.
*No reference : A pure logical Imagination.
Next query in queue : Are we sure , the statins,Rapathas & Inclisarans always reduce only the bad LDL ? (or it may reduce good LDL as well and give us a pseudo sense of bliss)
Before going into the topic, let us make it clear what is the real cut-off point between an embryo and fetus. All standard literature indicates an embryo becomes a fetus at the beginning of the 9th week when organogenesis, is to a large extent, completed. Ultrasonically, Crown-rump length > 35, beyond Carnegie stage 23, etc are used . But, practically, I think we have extended it up to 12 weeks, i.e., the first trimester. By this time, the fetus assumes a human shape in all aspects, moves the limbs, head, spine erect, eyes open, etc. Getting deep into this, the time-based cut-off definition is obviously not ideal. The errors of counting from the day of conception vs LMP is a big confounder in the published literature.
This may appear an non- issue , for most obsterticians , but specifcally in warfarin related embryoapthy , timing is everything*. Warfarin targets late embryo-to early fetal phase. (6-12weeks) This issue becomes very practical, when a pregannt women on prosthetic valve with warfarin reports to an obstercian at 10 weeks . Will he/she take a risk of preventing final phase of fetal warfarin related injury vs Heparin switch related prosthetic valve obstruction? (Ofcourse the Heparin bridge seems to have collapsed in most high risk thrombotic clinical settings. )
*Realise for fetopathy, there is no timing issue .It affects entire pregancy after 8 weeks.
Mechanism of Warfarin Embryo-fetopathy
Warfarin inhibits vitamin K epoxide reductase blocking gamma-carboxylation of proteins like osteocalcin and matrix protein, leading to skeletal defects in the classic embryopathy window (weeks 6-12). This is a biochemical not genetic or mutational defect . In the fetus, the side effects are due to its intended action, ie exccessive bleeding.
Warfarin Embryopathy
Warfarin Fetopathy
Timing of Exposure
Primarily first trimester (typically 6-12) 6-10% risk with first-trimester exposure
Second and third trimesters (after week 12) The exact incidence of fetopathy not known.it can be up to 25 % if we include all spectrum from minor CNS defects to still births. (Surprising there is a need for more data capture in this )
Mechanism
Primarily bio-chemical : Affects cartilage and bone formation via inhibition of vitamin K-dependent proteins like osteocalcin
Related to anticoagulation effects leading to hemorrhage, as well as CNS and developmental disruptions in the growing fetus
Clinical Features
Nasal hypoplasia Stippled epiphyses (calcified spots on bones visible on X-ray) – Skeletal abnormalities (e.g., short limbs, brachydactyly) – Facial dysmorphism –
Structural birth defects .Not dose-dependent beyond a certain threshold
Hemorrhagic and growth-related complications; more dose-dependent, with lower risks at low doses < 5mg
Is there a overlap betweeen embryopathy and fetopathy ?
Obviously yes. If exposure occurs around weeks 9-12 (early fetal stage), it could contribute to both structural anomalies (embryopathy-like) and hemorrhagic risks (fetopathy-like). Continuous or exposure across trimesters results in a combined phenotype, sometimes referred to as “fetal warfarin syndrome” (FWS), with mixed skeletal and CNS defects
Warfarin risk profile with reference to time : Is first first 6 weeks warfarin absolutely safe ?
It seems so. There is no evidence for any defects in preganct women taking htis in the first 6 week. It is a paradox like because almost 3/4 th of embryonal period , warfarin exposure is safe. Tihs satement is can be perplexing , as trnstion perios of embti to fetus is stull not clear and it is ot uniform in all . It aslo assumes embrys dont have cartialge so vitamin k is safe
Warfrin dose : Low vs high dose risk ?
Dose plays a role too: Low-dose warfarin (≤5 mg/day) reduces fetopathy risk but doesn’t eliminate embryopathy risk. The overall incidence of FWS (combining both) is estimated at 4-8% with warfarin use in pregnancy, with higher risks if exposure spans multiple periods. The much-celebrated 5 mg warfarin cutoff for safety, adopted by most advisory committees, requires a relook.
Warfarin effect on cardiac develoment ?
Wrafarin is well recognised to cause VSD, PDA , but rarely cono truncal anomaly.This explains the warfarin doesnt interupt early cardaic development and looping that stastrs at 4 weeks. The final septal sealing which happens in 8 the week is affected.
Acitrom is almost doubly powerful. 2.5mg of Acitrom is equal to 5 mg of warfarin. Acitrom has a half-life of approximately 10 hours. Because of this shorter duration in the body, stopping the medication and administering Vitamin K allows for a quicker reversal of the bleeding risk compared to longer-acting agent like warfarin.
1.Though we have strictly defined the time line between embryo and fetus (end of 8weeks) we are not clear when exactly the embryo, begins to synthesize cartilage and try to become a fetus.
2.The side effects of warfarin are purely bio-chemical and not due to genetic interruption or mutations. 3.To be more precise, the embryo is affected during it’s late phase, not in the first 6 weeks. 4.Low dose Warfarin is safe for the fetus, but not for the embryo. (The popular 5mg safety net is for optimising the risk, not for elimination)
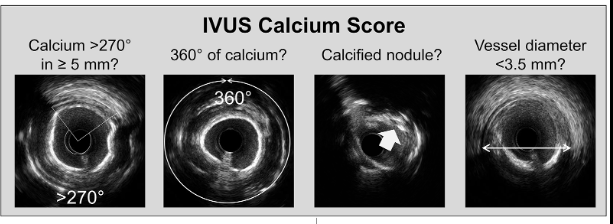
Intra coronary calcium : Are they really pro-thrombogenic ?
A.Yes
B. No ,
C. Yes & No ,
D.Don’t know ?
If you had answered either A or D , you may read further.
Calcium in the coronary artery is usually in the intimal/medial plane. It is covered by fibrous caps of varying thickness or just a single endothelial layer. Thus, calcium is not exposed to blood directly. Even if it is exposed, as in an eruptive nodule, the formation of thrombus is not attributed to calcium per se but to the exposure of subendothelial tissue factors .
1.If calcium is directly exposed to blood, does it trigger a clot?
Yes is the answer from most of us and even from pathologists. But the proof is vague. If that is the case, every degenerative, calcific aortic or mitral valves must form recurrent thrombosis. Thrombosis over these calcification are very rare , with 7500 liters blood traverse over it every day. (Now you know, why your answer was wrong)
2.Is it not true, calcium is essential in the clot forming process ?
Yes, Calcium is essential for the blood coagulation process. It is required for several key steps in both the intrinsic and extrinsic pathways, acting as a cofactor for the activation of various clotting factors.
Please mind, this free calcium is totally different . They are ionized calcium circulating in the blood , always charged to bind with a clotting factor.
3.Then how calcium is not pro thrombotic ?
Read below
4. Is the calcium in the blood and deposited Calcium Different?
Absolutely. The calcium that takes part in the coagulation process is free ionic calcium. Deposited calcium, within arterial plaques, valvular calcifications, is fundamentally different. It exists primarily as insoluble crystalline compounds, such as hydroxyapatite (a form of calcium phosphate) which is the same mineral found in bone. This is a solid, bound form resulting from dystrophic or metastatic calcification process. The are largely Bio -Inert atleast with reference to coagulation.
Final message :
Coronary calcium, whether within the tissue plane or exposed to the lumen, is not directly thrombogenic. They are dead-end inert products of atherosclerosis. However, the prothrombotic trigger occurs with some of the sharp calcium crystals or nodules when they injure the endothelium and expose the subendothelial tissue factors. Abluminal endothelial injury from the intimal calcium is far less common* in most chronic CAD, unless , some aggressive humans decide to wage a intra-coronary calcium warfare, to facilitate stent deployment .
*Disproportionate calcium loading in the shoulder region of the plaque can make a plaque vulnerable. Having said that, overall in a holistic atherosclerotic landscape, calcium is more of an enemy of cardiologists, who face a hurdle to place stents than the patient who harbor it..
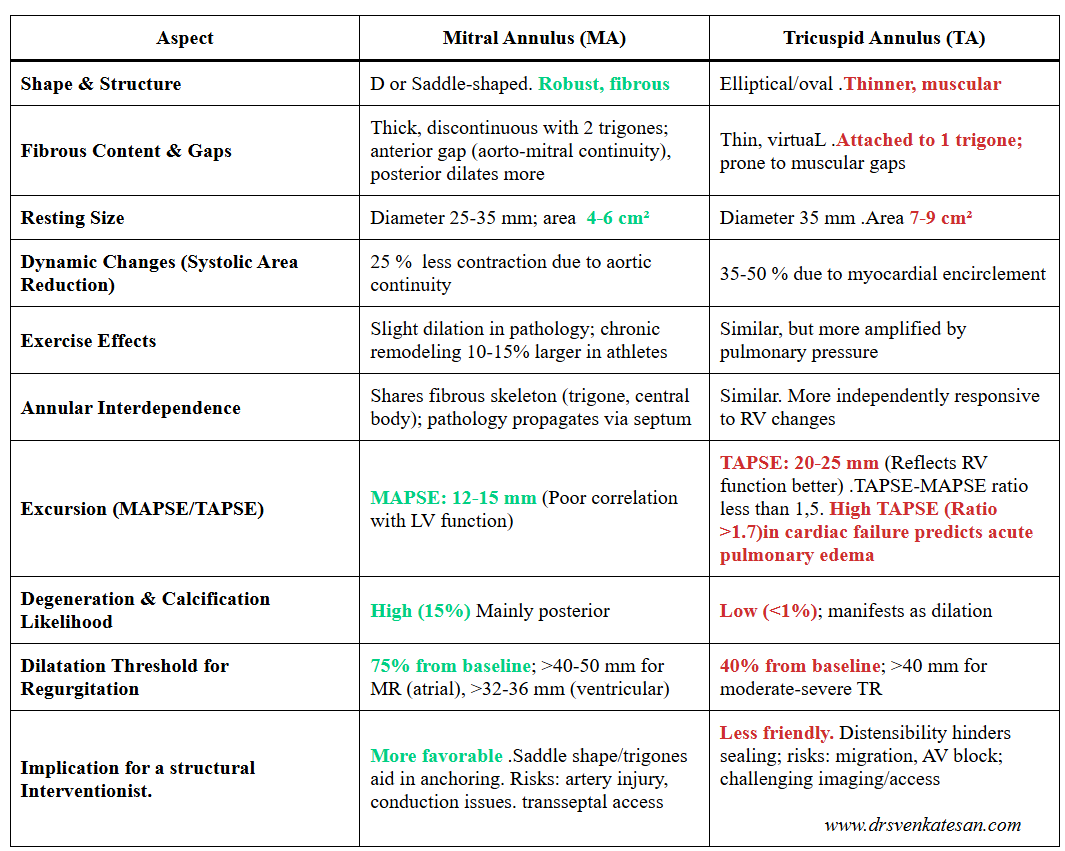
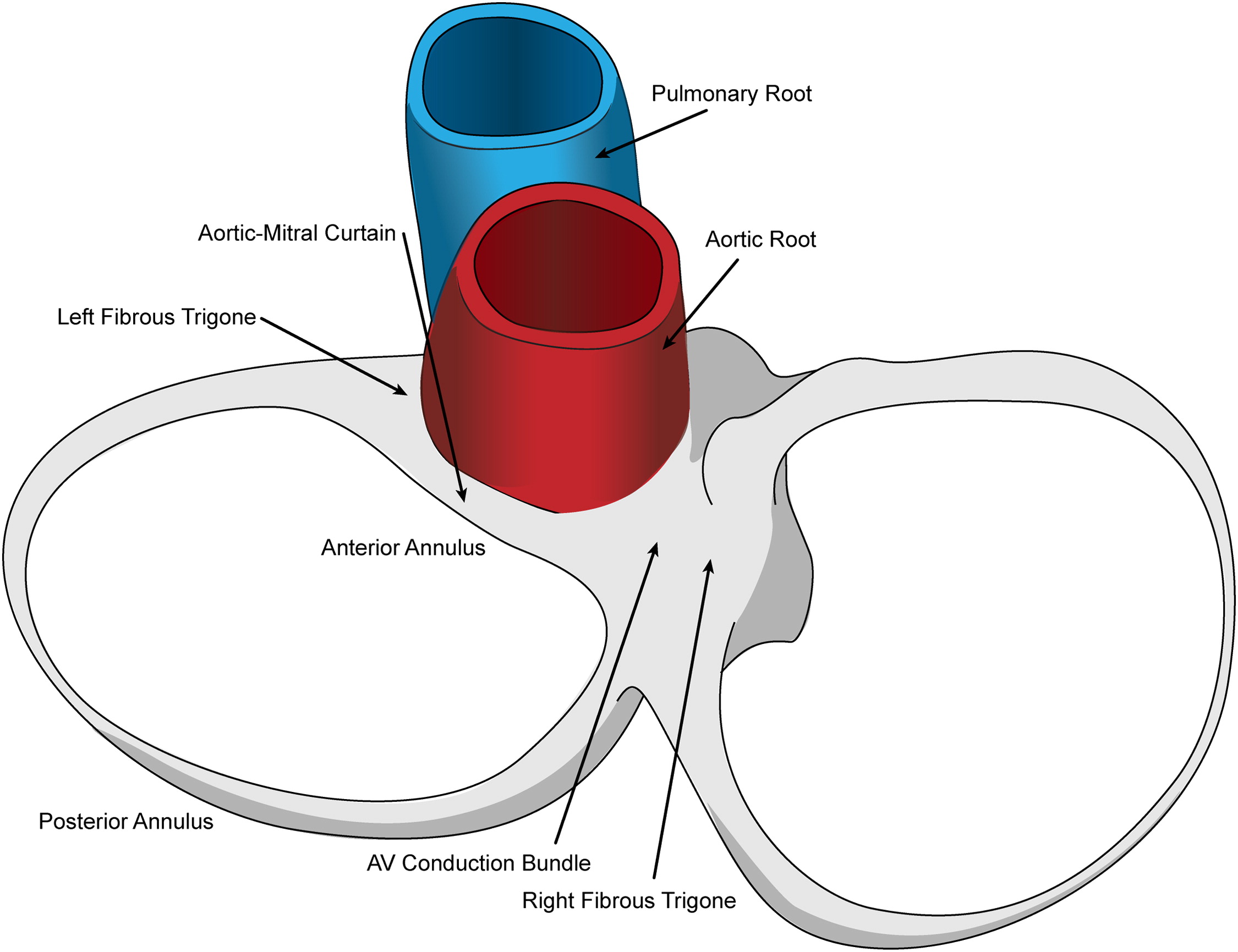
The table was gathered with content from multiple sources and few personal observations. Any doubts please check with more authentic sources. To understand fully, we need to read extensively the anatomy of the cardiac fibro-skeleton. (Saremi F, . Radiographics. 2017 )
Image source: Mitral Annulus: An Intraoperative Echocardiographic Perspective Mahmood, Feroze et al. Journal of Cardiothoracic and Vascular Anesthesia, Volume 27, Issue 6, 1355 – 1363
Final message
One important message we get is, the tricuspid annulus is more dynamic despite it being attached to a low-powered chamber. The second clinically important lesson I learned was, if the RV annulus doesn’t balance its motion corresponding to its mitral counterpart, there is a risk of developing more pulmonary congestion in a compromised heart with LV dysfunction. What can be refered to, as un- balanced Bi-Ventricular failure (The TAPSE to MAPSE ratio explains about this : Zhang H, BMC Anesthesiol. 2023 )
Postamble
After going through the reference article cited below, it is fascinating to realize the cardiac skeleton is just like a fragile fish bone hidden within the heart, to which all the vital structures, right from the muscles ,valves, and even the great arteries are attached with varying degrees of firmness. Wonder, it ever gets fractured ? may be in most degenerative heart disease like Lev’s or Lenegres.
It is not at all a secret, among the four heart chambers, right atrium receives the least attention from cardiologists, as it is perceived merely as a conduit for venous return. (Why we forget, the fact? that the same blood that is handled by RA, would become the left ventricular stroke volume few beats later) .
Ironically ,”a” wave in the neck is celebrated for over a century as a evidence for a brisk and forceful contraction of RA. Meanwhile we also observe, with the onset of atrial fibrillation (AF) there is no dramatic hemodynamic deterioration in most people, reinforcing our assumptions might be correct after-all ! (Which is not)
So, we must admit , we have some difficulty to understand the true power of right atrium. But, as now, as on 2026, we begin to realize RA’s role is central in filling the RV, and thereupon the Pulmonary circuit and LA. It is also not clear, why RV frank starling law is rarely considered important, in spite of the fact, RV wall stretch is directly dependent on RA volume.
What is normal RA volume ?
(See below) Technically every chamber must have stroke volume plus something , that will remain as residual after its emptying. In that sense, RA volume is about 100 ml. (During exertion, it can go even to 150 ml). One curious issue in the morphometrics of RA is, unlike the other chambers, the inlet boundary for RA is vague as IVC and SVC simply blends to form a tubular chamber without any valves. During peak exercise, one may not distinguish the physiological limits of the inlet of the right atrium.
Table taken from Ref 1 . Note : There is something called RA ejection fraction. Might be of immense importance in right heart failure.
What happens to RA volume in cardiac failure ?
It is no surprise, the thin-walled RA enlarges more than RV. Also, in the chest X-ray, the cardiomegaly is significantly contributed by RA rather than RV.
Note the relationship between RA volume with RV dysfunction .
Clinical implication of RA size and function
*As on the left side, we have right atrial functional TR , worsening the RV function in vivious cycle.
*We are in the era of TEER and Percutaneous bio prosthetic tricupid valve. Unlesss we assess the intrisic fcuntional integity of right atrium , we may not be able to get optimal out come .
*More recently consensus conference on pulmonary hypertension, which was adopted by ESC, has included RA area with a cut off 18sq.cm (It should have been volume ideally) as an indicator of PH (Fischer L,. Respir Res. 2018 )
Final message
For cardiologists, LV will remain the emperor of the Heart. RV and also LA are also receiving enormous attention. Sadly RA is hidden in a discriminatory blind spot. It is ironical that we sort of give more respect, even to IVC and SVC flows than RA dynamics. I think we may have to pay a price for it if we continue to neglect it. It may take more time for us to study the right atrial mechanical function and its ability to overcome the dysfunctional right ventricle (RV diastolic dysfunction).
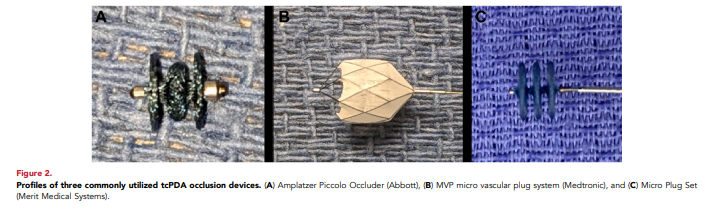
Transcatheter PDA (tcPDA) closure has become the preferred invasive option for hemodynamically significant PDA (hsPDA) in preterm infants after the recent FDA approval of dedicated devices . However we need to ensure that this powerful therapy is used selectively, based on true hemodynamic need, with proper expertise and infrastructure, and not as a routine response to any persistent duct. SCAI has come out with a new Position statement on this issue. (Ref 1)
Prematurity, PDA, and hemodynamic significance
Extremely premature infants have a high incidence of persistent PDA and are vulnerable chronic lung disease, pulmonary vascular disease, higher respiratory support, NEC, and mortality. Not all PDAs in this group warrant closure .Treatment is strictly reserved for hsPDA, where the left‑to‑right shunt clearly causes pulmonary overcirculation and/or systemic hypoperfusion. It is wise to note, medical therapy closes about two‑thirds of PDAs versus about one‑third without treatment, underscoring the importance of pharmacologic management alone.
Recognition of significant PDA : Clinical or Echocardiography ?
It is prudent, the selection for tcPDA should start with clinical assessment. It mainly goes with high ventilator or oxygen dependece attributed to shunt physiology, plus signs of systemic compromise despite optimal general care. Infants <28 weeks’ gestation, >10 days old, and still invasively ventilated in high‑risk units are potential candidates when these clinical features are present and expertise is available.
Limits of echocardiographic Indices
Echocardiographic parameters include, duct size, left‑heart volume loading, and holodiastolic flow reversal to define hsPDA . It must be emphasized Duct diameter alone correlates poorly with true hemodynamic impact. A large PFO or small ASD can decompress the left heart, blunting classic echo markers and masking a genuinely important shunt . Also , dynamic pulmonary vascular resistance, sepsis, systemic inflammation, renal dysfunction, may exaggerate the severity of an anatomically modest shunt, leading to unnecessary catheterization.
Pharmacologic closure with ibuprofen, indomethacin, or acetaminophen remains the recommended first‑line approach with a closure rate of 70% .
Final message
Transcatheter rather than surgical has become the definitive option when conservative or medical therapy fail. (Inspite of the fact, catheter access can be difficult in very small babies ) .However, the more important issue could be avoiding premature and unnecessary device closure in premature infants.
This is not a completely Imaginary conversation, between the wife of a recently discharged STEMI patient and his cardiologist. This happened in a top ranked heart care center in my city Chennai.
Caution: Strong language
Patient’s wife :
Doctor, why my husband is suffering from significant LV dysfunction in spite of a timely & successful primary PCI. You assured me you are doing the best.
Cardiologist:
Yes, you are right. I am sorry, for that.
Patient’s wife :
But, doctor, on the day of discharge you told us proudly, the procedure is 100% success and you have relieved the block and restored blood flow. I recall, you quoted some Tomy score, and all.
Cardiologist:
Yes I did. It is not Tomy, it is TIMI 3, which we use routinely, and … to be frank, it actually means nothing. It tells us, we have restored flow across the artery at the site of block . It can never guarantee, all those blood, will reach the ailing muscle.
Patient’ wife:
TIMI or TAMY, doesn’t mean anything to me doctor, It sounds like my neighbors’ pet. All I want to understand is , whether the procedure was really successful. Yes or No ?
Cardiologist:
You are correct. I am extremely sorry. It is really an Incomplete myocardial salvage. Your husband’s myocardium is significantly damaged. You must also understand , these things are not in our hands. It is the destiny that decides the fate of the myocardium. It lies deep in the myocardial microvasculature, which doesn’t obey our conventional time windows we talk about.
Patient’s wife:
That’s ok. But, what is the need for mis-communication to us. Why didn’t you admit it as a failed primary PCI in your discharge records ?
Cardiologist:
I agree with you. But, scientifically it is not a falsehood. For us, it is still a success, because we are just macro-vascular cardiologist. We define success based on removing blocks, not the true myocardial reperfusion.
Patients wife:
That’s awful. Sorry, for being harsh .For heaven’s sake please go and change your horrible definition for a successful PCI ,in the cardiology literature.
Cardiologist:
Thanks for bringing up this less discussed entity “Failed primary PCI” We rarely discuss about it (In the biased minds of interventional cardiologists, only thrombolysis can fail). Surely, we will pass on your genuine concern to the concerned authorities.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.
 Calcium is essential for the blood coagulation process. It is required for several key steps in both the intrinsic and extrinsic pathways, acting as a cofactor for the activation of various clotting factors.
Calcium is essential for the blood coagulation process. It is required for several key steps in both the intrinsic and extrinsic pathways, acting as a cofactor for the activation of various clotting factors. 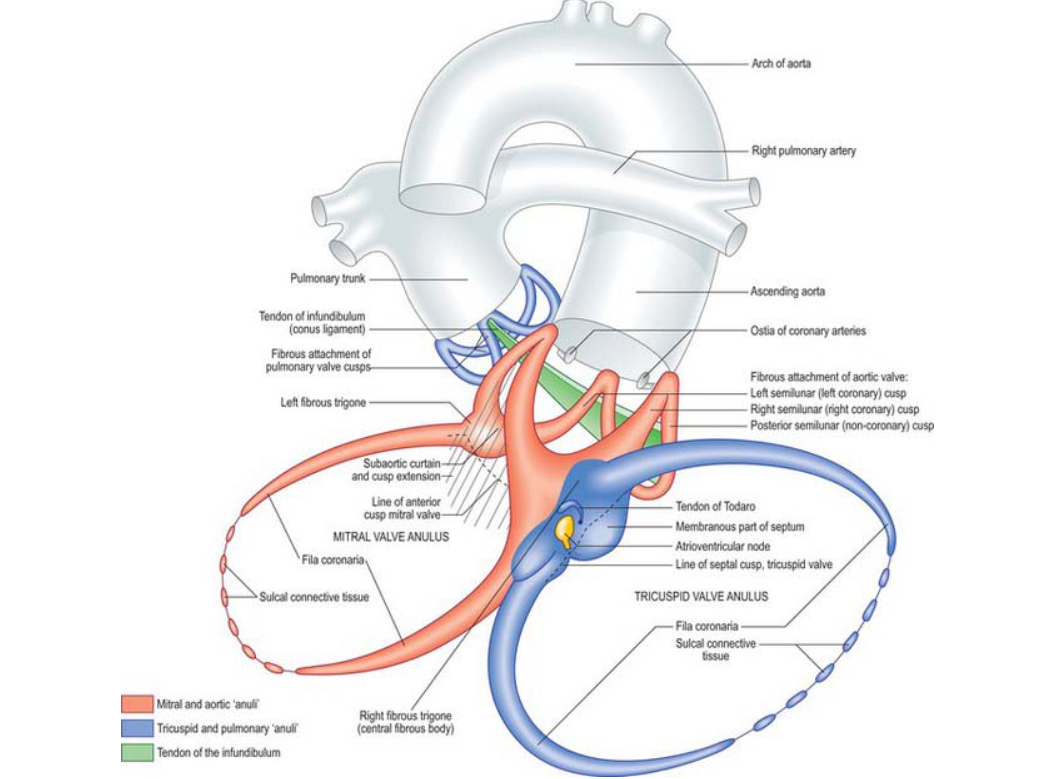







{kind=link}