Simple answer : If one leaflet is absent (True embryonal agenesis of anlagen) then corresponding sinus also fails to germinate. So number of leaflet is equal to number of sinus.This implies,In normal Tricuspid aortic valve there are three Aortic sinuses. In Bi-cuspid Aortic valve there are two Aortic sinuses depending on the absent leaflet (Generally R & L sinus present)
But, reality is complex : (Apparently , there can be no relation between the leaflet and cusp) Here, a distinction is made between truly absent leaflet to fused BCAV. In fused BCAV (ie with or without raphe )the number of sinus can be three like a normal Aortic root .
Is fusion line same as Raphe ?
Usually yes. Raphe is a raised ridge which is a marker of fusion plane But, cardiac morphology never allows us to take things easy. To complicatt our thinking, the fusion can be smooth and perfect without a ridge or raphe. This raphe less fusion makes it difficult whether we are dealing with true geno-phenotypically BCAV or simply fusion phenotypes of what should have been a genotypic- tricuspid valves . There is a simple clue in this complex scenario .In the later case it is identified by presence of three sinus. Does this make simple our understanding right ?( I am not sure, the above understanding is correct , this is how I Interpreted. (Please, clarify if some one finds it wrong)
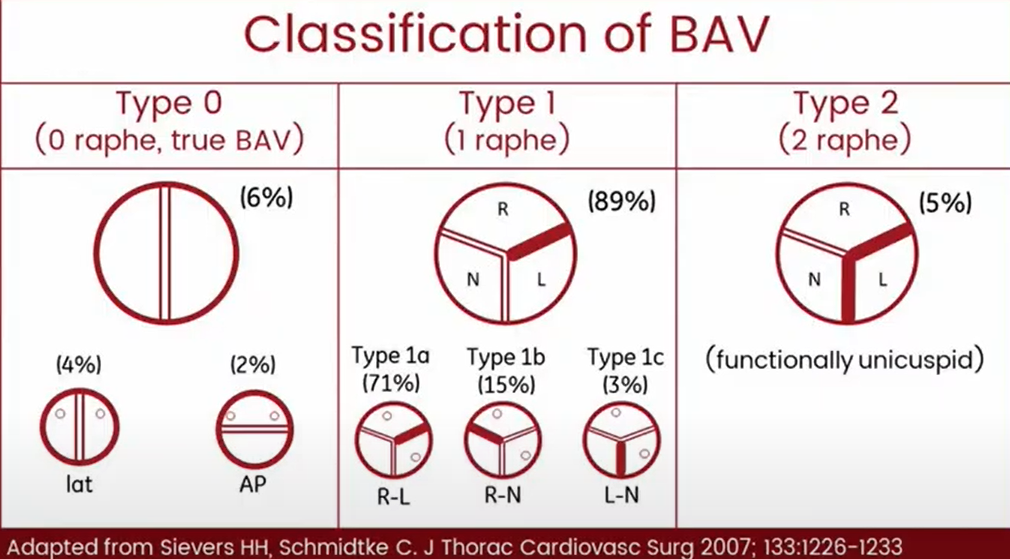
The two famous classification of Aortic leaflet 1.Siever 2.Micahlena
Why is the number of cusps important ?
It decides the type of TAVI valves and location of implant.
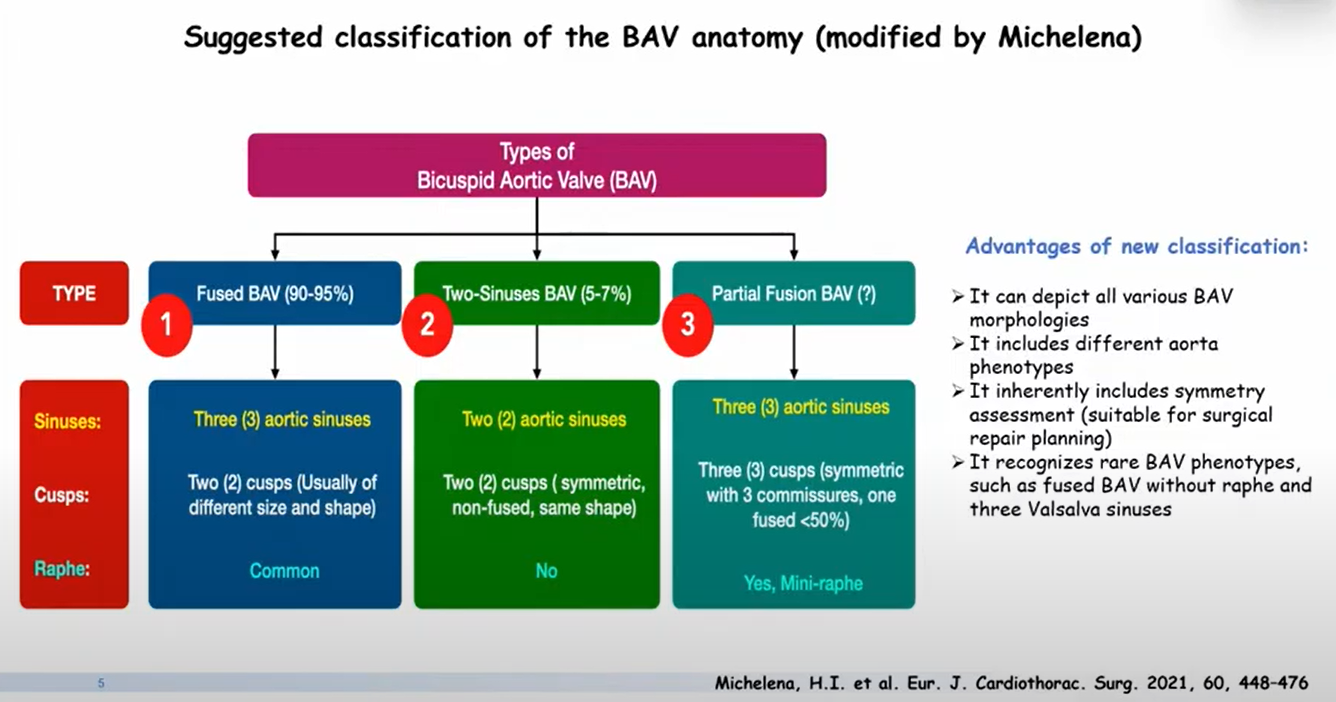
Fortunately, we have a consensus nomenclature system for Aortic valve leaflets
- BCAV types are defined as fused BCAV,
- Two-sinus BCAV,
- Partial-fusion (or forme fruste) BCAV.
The fused BCAV type is the most common type (90-95% of BAV cases); and is characterized by two of three cusps appearing fused within three distinguishable sinuses of Valsalva; frequently but not always with a congenital fibrous ridge (raphe) between the fused cusps.
- Right-left fusion is most common (70-80%). The right-left phenotype also is most common across all variations of aortic valve dysfunction (AS or AR) and aortic phenotypes (normal aorta, dilated root, dilated ascending aorta, dilated arch).
- Right-nonfusion is second most common (20-30%), and in adults is associated with a higher prevalence of AS and of progressive AR.
- Left-non fusion is least common (3-5%).
The two-sinus BCAV type is uncommon (5% of BAV cases), with two cusps of roughly equal size within two sinuses of Valsalva.
- Laterolateral (side-to-side) two-sinus BAV has one coronary artery arising from each sinus.
- Anteroposterior (front and back) two-sinus BAV can have one coronary artery arising from each sinus or both coronaries arising from the anterior sinus.
The partial-fusion BCAV ( forme fruste) type is more recently recognized and of unknown prevalence. The appearance is similar to a typical tricuspid aortic valve, but with <50% fusion between two cusps at the commissural base forming a mini-raphe.
Next query :
What are differences between raphe and commissure ?







