Fixing the target LDL, in both primary and secondary prevention is becoming more & more complex . The reason being, there is a huge healthy population ( with zero risk factor) , but showing insignificant or minimal coronary plaques. This subset of population is anxiously unmasked by inclusion of CT angiogram in many master health check-up programs.
A case profile & a debate
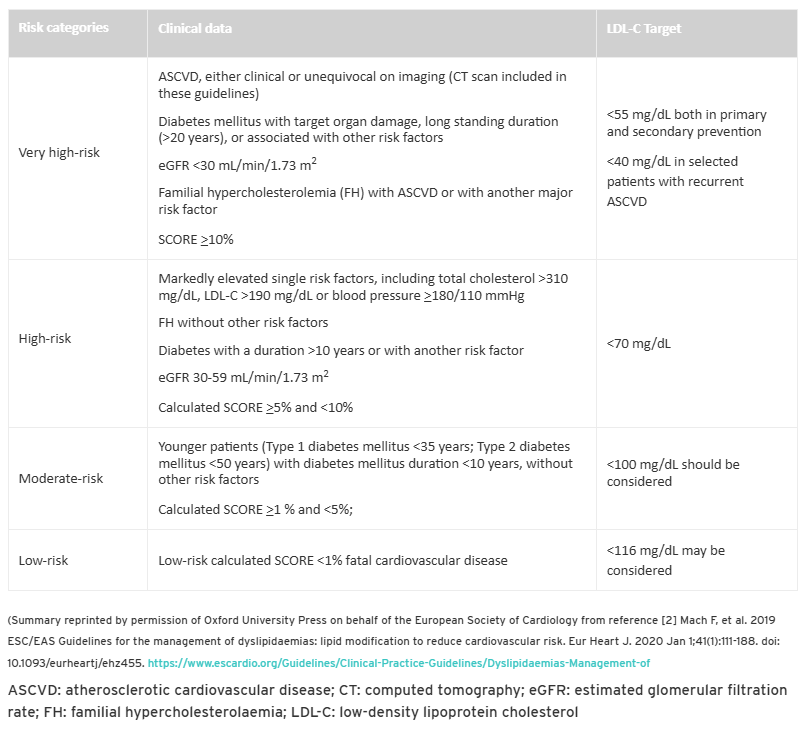
What does the guidelines say ?
If you have any athero-sclerotic cardio vascular disease(ASVD) documented by clinical or Imaging , you belong to very high risk category. It clearly says the target is 55mg both in primary and secondary prevention.
LDL is not only the enemy of the coronary artery. Fatty streaks in the coronary artery begin in the fetal stage itself. In adults, some of these streaks become prominent locally and turn out to be plaque. The argument for intensive statin therapy is to stabilize these plaques. We would not know if the plaque is stable or not. We can’t do OCT imaging, an invasive test, to know about the vulnerability. So, for the sake of safety, everyone advises intense statin therapy. The irony is ACS continues to occur at any level of LDL.
Final message
Is my cardiologist right about the LDL target of 55 mg ?
If you look at the above table of risk categorization, your cardiologist may be right. But the deeper issue is whether such a recommendation is correct or not. In our opinion LDL 70mg is good target to achieve. Lowering further, has its own risk. I am sorry, you can’t escape from the guidelines as of now, Further you don’t have any other risk factors to treat as well. Then, this question, will always hang above your shoulders , why the hell I got this plaque over there?
I think ,its time ,we need ask more questions that are difficult to answer ?
1.Does ASVD includes even 10-20 % plaques by CT angiogram ? How specific these X RAY – stitched slices of CT scans done on moving heart. Then ,what about luminal irregularities ? Should it to be counted as ASCVD as well ?
2.Do we need to refine the definition of by introducing a new term significant ASCVD?
3.Also like subcategorization of clinical ASCVD from image-based ASCVD with reference to target LDL?
Reference
Postamble
Dear patient, wait, there can be more shocking advisories soon. With the famous PREVENT trial (Lancet 2024), results are waiting on the sidelines trying to penetrate the fragile barriers of various guideline writing committee offices. By the way, PREVENT study demands an OCT for all non-flow limiting plaques, and stents if they are found be vulnerable.( Read about The TCFA story)