The prime job of cardiologists is to restore coronary blood flow in an emergency fashion. While we do this with reasonable success ,there is still a missing link between our Initial aim and achieved goal.
It’s all too common situation in any busy cath lab , to see two similar STEMI patients with identical time window & proximal LAD as IRA , in totally different scenarios. In the first patient we find a trickle of flow in LAD , who is relatively comfortable with normal LV function (In whom , emergency primary PCI might appear redundant.) While the other patient , even after rapidly established TIMI 3 flow , LV wouldn’t look good at all . All our efforts to reperfuse is found wanting. Ultimately LV goes in a downward spiral , ends up in irreversible cardiogenic shock or fatality inspite of Impellas, ECMOs and other LV assist exotica !

I can promise , you can never guess from the angiogram whether this ACS patient was very much comfortable or he is in cardiogenic shock on ventilator unless I reveal the history. Am I right ? That is the mystery of coronary circulation and hence its so critical to serve the myocardium what it wants ? Never treat a coronary artery in isolation !
What is the possible explanation ?
The first trickle (Say TIMI 1 which is usually spontaneous or lytic related ) is the one that’s going keep the muscle viable and possibly prolong the time window for the subsequent reperfusion strategies .Hence it is the timely TIMI 1 or 2 is much more critical than delayed TIMI 3 (Still rapid).
Time window woos :
Who fixed the reperfusion time window as 6 to 12 hours ? Do you know on what basis the acceptable delay of 30 to 60 mts related to primary PCI ? was made acceptable by cardiology community ? If you analyse the published data both are highly contentious and empirical. ( Suggest you scrutiny the data from DANAM2 , PRAGUE and AIR PAMI and come to your own conclusion) (*These are the 3 sacred studies done with few thousand patients that redefined our approach to STEMI and gave the licence to waste the golden hour ! )
I remember reading the Robins pathology book (Bible of pathology William Boyd as well ) in early days of medical school myocardium may die even within 1 hour with wavy necrosis, contraction bands etc. Looking back some times I wonder how the clinicians have conveniently prolonged time window with whims and fancies of science Intact.
Concurring with the pathologists , we have learnt some harsh lessons inside the cath labs. One of them is that even ultra fast pPCI can fail to salvage myocardium, meaning that time is not the ultimate thing in our race. (There should be other important determinants )
A brief journey back into our pathology classes : Have a look at this table
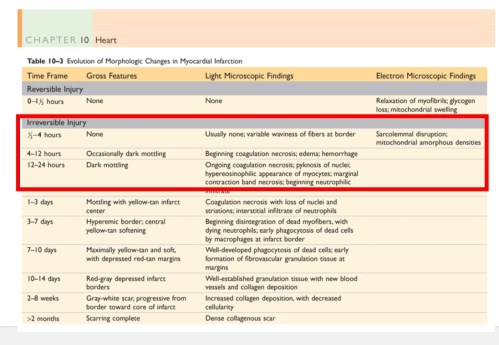
Please note, Irreversible Injury might happen any time after 30 minutes .Of course it can vary . But, the question is how are you going to identify these patients with ultra short time windows? source : Robbins Basic Pathology 9th Edition.Elsevier
Other factors that influence myocardial cell survival
- Tendency of myocardium becoming electrically unstable
- Criticality of non IRA lesions
- Ischemic preconditioning
- Gender dependent reperfusion times
- Efficiency of collateral circulation
- Reperfusion Injury (R.A. Kloner, Ultrastructural evidence of microvascular damage and myocardial cell injury after coronary artery occlusion: which comes first?)
- Co-morbid conditions
Re-perfusion is not a single edged sword
We may wish the concept of re-perfusion Injury is a myth : Unfortunately it is not ! Myocardium doesn’t relish (not always) the return of circulation in full dose. (May be it’s laying and taking the much needed rest with the initial Injury!)
Sudden gushes of blood leads to extravasation into the interstitium (due to damaged capillaries) increases the Intra myocardial resistance and obstructs the microvascular flow. We have witnessed more than a handful of patients going for cardiac arrest once IRA is opened (of course, we might be able to resuscitate many of them )
Myocardial hypoxia resistance time
Please realise ,true STEMI clock starts not with onset of symptoms but with time of total occlusion.There is more than subtle difference between the two. Onset of total occlusion to symptom time is not a well explored or understood Interval. We take it for granted that the onset of symptoms coincides with total occlusion.
But in multi vessel CAD, even a CTO can cause a STEMI through loss of distal collaterals. Further ,the presence and absence of pre-infarction angina (PIA*) , ischemic pre-conditioning (IPC*) sensitizing effect of remote CAD , manifest vs recruitable collaterals all these make the fixed time windows with which we did our land mark studies of PCI / lysis academically questionable.
* Both PIA IPC are master confounders in the true time window calculations .We don’t know whether its due to ischemia tolerating myocytes or pain tolerating nerve fibres responsible for this varying presentations.But the mystery is certain , when we realise the angiographic spectrum of ACS can range from silent ATOs to painful CTOs
Final message
Is timely reperfusion (and its favorable effect ) lies in God’s domain ? If you we believe myocardial susceptibility , arrhymogenicity and recovery to hypoxia is genetically determined ,then the difference between fate and science Is much narrower than we think .Its appears we can change the former with the later with both positive and negative outcomes. So ,the “f” word may not be a forbidden at-least in the STEMI management. It resides not only within the human genomic codecs written with double-helical nucleic acid fonts . . . but also in the nimble and restless hands of both novice and experienced interventionists !
A study proposal
Let me make a hypothetical statement .A significant subset of patients with STEMI have ultra short myocardial survival and we are unable to identify these hypoxia challenged hearts where primary PCI related delay could be a myocardial sin. Any one willing to prove or disprove this hypothesis ? If some body take this quixotically important study in STEMI management please give me some credit as a contributor !



