In the evaluation of syncope, history is most important to arrive at a diagnosis. Ofcourse, the first step is to confirm whether its truly a syncope or something else.(Metabolic/TIA or seizure.)We are easily carried away by the urge to order a Holter monitoring routinely. In reality, the yield is too low (<15%) .Even the utility value of Head up tilt (HUT) is being downgraded.
Paradoxically, resting ECG might give important clue in many. One need to specifically look into a set pattern of ECG. It generally falls in one the following in any patient with syncope.
This post specifically may not be exclusive but stresses the importance of resting ECG in the evaluation of syncope. by our urge (Stress testing is not included)
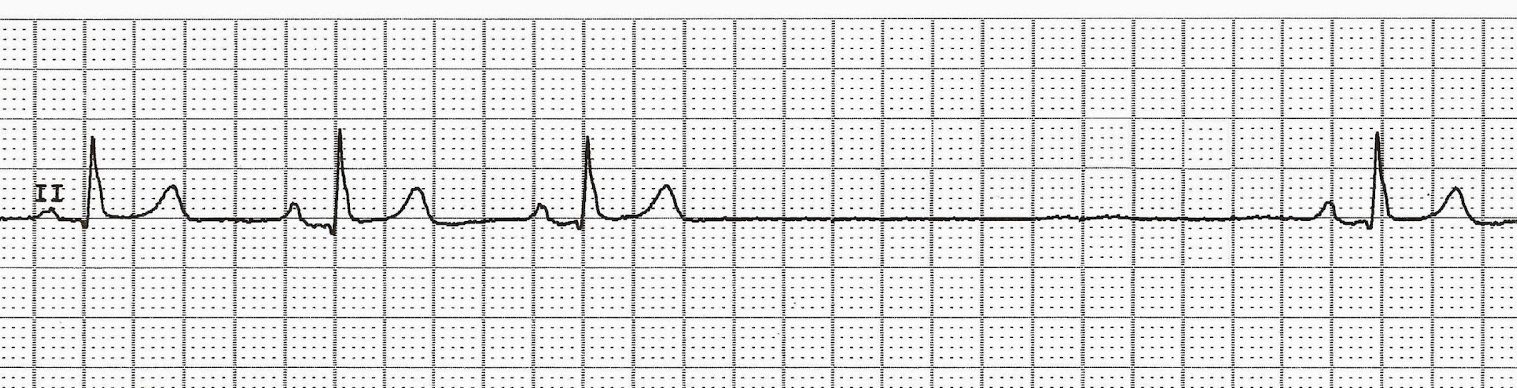
- Bradycardia( Sinus Node dysfunction/AV block) Note Brady cardias can per se cause syncope if pause >3-5sec Or it may lead to Brady (Pause) dependent escape VT.

A pause can be a sinus arrest, Pause or SA block .If pause ends with a junctional escape it becomes a arrest.
- Look PR interval specifically(A bifasicular block shouldn’t be missed .It can be more dangerous than say a congenital CHB)PR interal represents condcution from SA node to Purkinje fibres in ventricel. The importance is directly linked to the location of the block than propably the degree of prolongation. Please note HV interval > 70 ms in any patient with prolonged PR is cause for concern,
- Preexcitation/Delta waves (Though Narrow QRS AVRT rarely causes syncope its very much possible during Antidromic tachycardia. (AntiVRT), Antidromic AVRT or Accessory pathway with short RP <250ms need to be documented. Concealed paths are safe , but delta appearing during stress testing is extremely unsafe
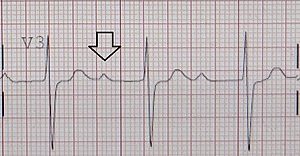
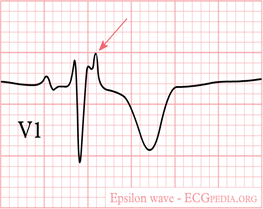
- Post-excitation /Epsilon waves. (often noted in lead V 1, A marker of RVOT dysplasia as in ARVD. Also referred to as Fontaine wave who discovered it by bipolar cheat leads over V1 )
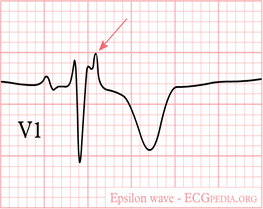
Note the epsilon occurring after the qrs Indicating RVOT dysplasia
- Q waves (Markers of old MI -Scar Induced VT)
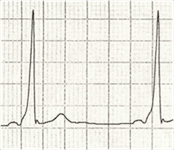
- High voltage QRS LVH /HCM /Aortic stenosis
- RV strain/S1Q3T3 pulmonary embolism.(Syncope is a common presentation with PE especially with minimal exertion or change in posture)
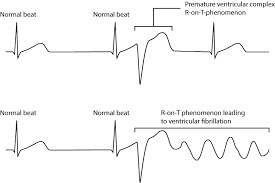
- Early coupled VPDS (R on T location a trigger for VT) Wedesky effect. The terminal portion of T which correspond to supernormal period.
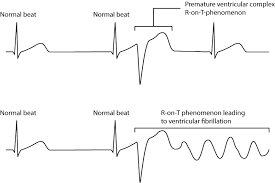
The significance of VPDs directly related to its prematurity than its focus of origin.The one that falls on the vulnerable period .Late phase 2 and phase 3 are more vulnerable as triggered activity
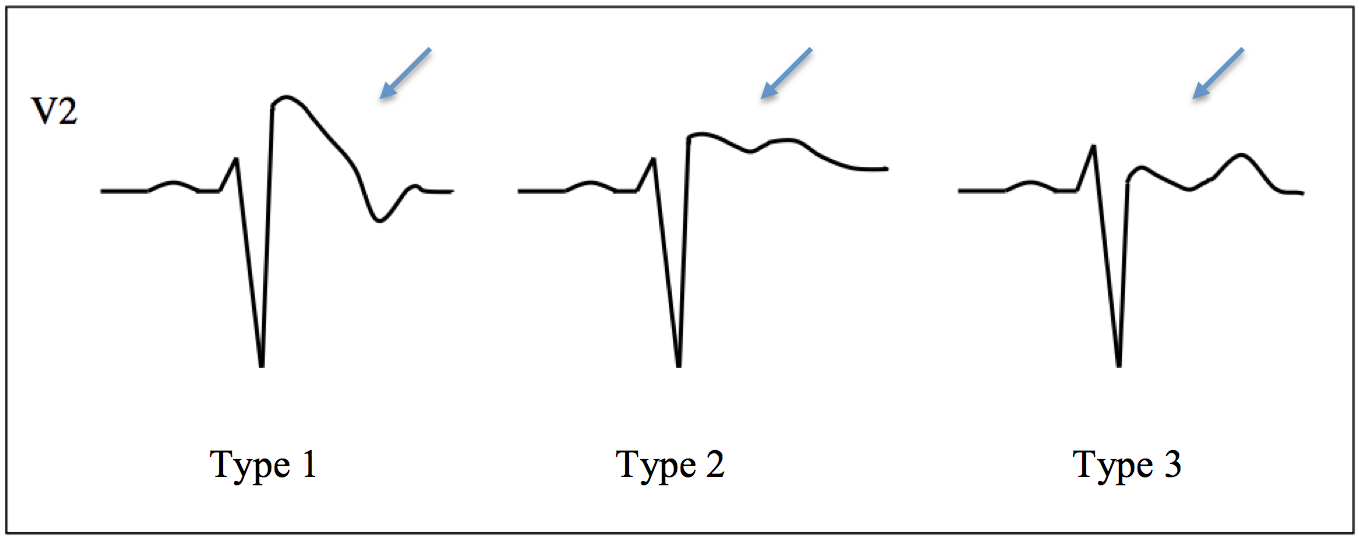
- Brugada (Type 1 with T inversion riskier, Camel hump less dangerous

Brugada syndrome -Note three types . Type 1 is typically risk prone. Please note it is the late ST declining component and the T iversion that confers the risk not ST elevation per se.The type 2 with a camel hump is confered with least risk
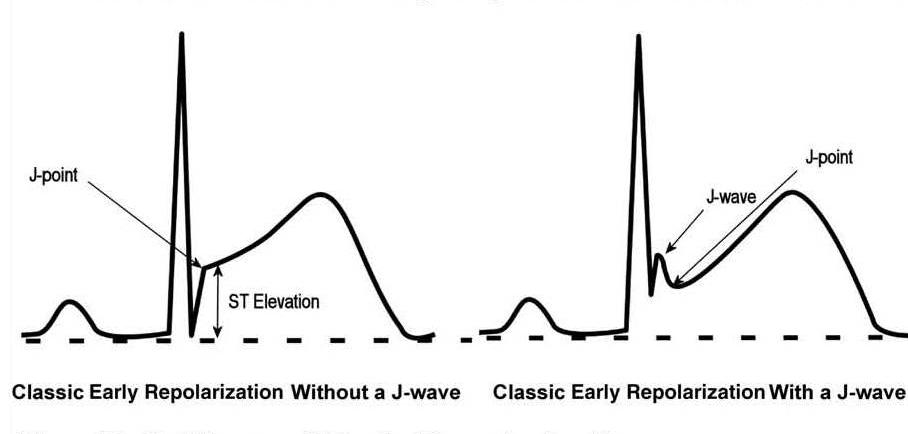
- Malignant ERS pattern (Most ERS or safe / Maligant forms infero lateral forms risky only at times of ACS not spontaneous risk
- J wave syndromes –Overlapping with Brugada /ERS Charles Antzelevitch,J Arrhythm. 2016 Oct; 32(5): 315–339

ERS syndrome are so common. In the absence of sycnope, it should be ignored straight away. Recently it received too much hype among cardiologists increasing the anxietywhich is not warranted.
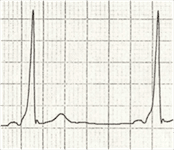
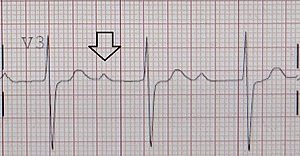
- Long QT Interval (Hypokalemia commonest, Congenital next ,Long-QT Syndrome Circulation: Arrhythmia and Electrophysiology. 2012;5:868–877
- Fractioned QRS (Most often seen in DCM ischemic /non-ischemic confer VT risk usually with LV dysfunction, these are candidates for CRT-P/D as well)
- T wave alternans Fluctuating T waves indicate repolarisation alternans .It elevates risk of VT Narayan SM J Am Coll Cardiol. 2006 Jan 17;47(2):269-81
- Exercise Induced VT/ CPVT is to be considered seriously in all unexplained exertional syncope. Behere SP, Catecholaminergic polymorphic ventricular tachycardia: An exciting new era. Ann Pediatr Cardiol. 2016;9(2):137–146.
What next after ECG ?
After ruling out neuro cardiogenic syncope by history, one has to perform a good quality echocardiography that can clinch structural heart disease .In cardiomyopathies like ARVD or RCM MRI studies will be of immense value especially the LGE/DEMRI that picks up the scars and fibrosis as in sarcoid or tuberculomas etc. Event recorders are popular, may have a slightly better yield than Holter.EP studies are required in few as diagnostic or more commonly as a part of therapeutics.(Please note, EP lab Induced polymorphic VT has Zero diagnostic value as any normal human heart can be induced to VF by repetitive stimulation)
Management
The main purpose is to exclude serious primary electrical and or structural heart disease. However, fortunately, the most common cause of syncope is neurogenic or reflex mediated. It requires reassurance and fluid repletion Fludrocortisone,/Midoridine (Alpha receptor agonists are promising) Pacemaker/ICD is indicated in few with brady/Tachy -Brady .ICDs/RF ablation are Indicated in Ischemic VTs channelopathies with inherited VT/VF like Brugada. One important question still not clearly answered is when to refer a patient with syncope to Electrophysiologist. ? For me , it appears only a fraction may need it.
Further reading (2018 ESC guidelines)




