I have never found it difficult to retrogradely cross a dangerous epicardial collateral in complex CTO. Delivering a twin stent in a partial culotte strategy for a bifurc lesion has never tested my talents. Stenting a left main across the LAD, jailing the LCX with OCT support is my favorite time pass. Crushing a calcium infested diffuse long lesion with diamond-tipped ablator appear as breezy as shopping in a mall.
But this one is really challenging
What is that?
Understanding these four studies (Ref 1-4 ). They dogmatically say medical management confers definitive protection in chronic coronary syndromes. It stretches our limits of Imaginary Intelligence! How can a near tight coronary obstruction sitting right across your eyes, be left untouched? The latest one seems to suggest we can even ignore FFR positive lesions.
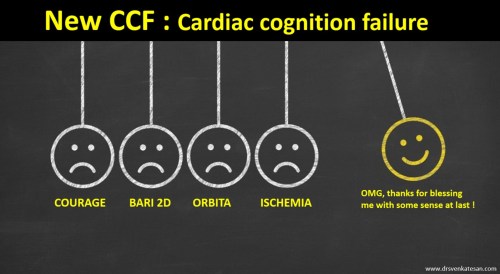
It requires 4 negative forces . . . to bring one big positive Impact!
I don’t understand who is funding these negative trials and glorify it, and trying to defame the talents in me. All these studies have a huge lacuna. They conveniently exclude high-risk cases and allowed liberal cross over to PCI later on. Even the just-released ISCHEMIA trial had 38 % patient with no angina. (But why they received PCI ?) How to Interpret these trials and extract the true conclusion? .One consolation is, I know these negative trials have a very short memory and expiry date. Very soon I shall be liberated from the clutches of this negativism.
Even as I scribble this, my inner conscious is telling a completely different story. I agree we do Indulge a lot in stable Ischemic Heart disease. (SIHD). I am yet to be clear what exactly we mean by SIHD. How is that near 90 % mid LAD guy ran 12 met exercise with negligible perfusion defect and still FFR was .7 ?
OMG, save me from this academic conundrum and help to acquire true wisdom.
Reference
1.Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurkovitz C, et al. For the COURAGE Trial Research Group. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008;359(7):677–687. [PubMed] [Google Scholar]
2.BARI 2D Study Group. Frye RL, August P, Brooks MM, Hardison RM, Kelsey SF, MacGregor JM, et al. A randomized trial of therapies for type 2 diabetes and coronary artery disease. N Engl J Med. 2009;360(24):2503–2515. [PMC free article] [PubMed] [Google Scholar]
3.Al-Lamee R, Thompson D, Dehbi HM, Sen S, Tang K, Davies J, et al. ORBITA Investigators Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet. 2018;391(10115):31–40. [PubMed] [Google Scholar]



