Having retired, find little more time in browsing the academic images lying idle in old computers.It is interesting, still a tiring job to pick any useful learning stuff, from heaps of data hiding in different hard drives.
This set of ECGs I could retrive from the year 2011, A 31-year-old male presented to our CCU at 4.50 PM.
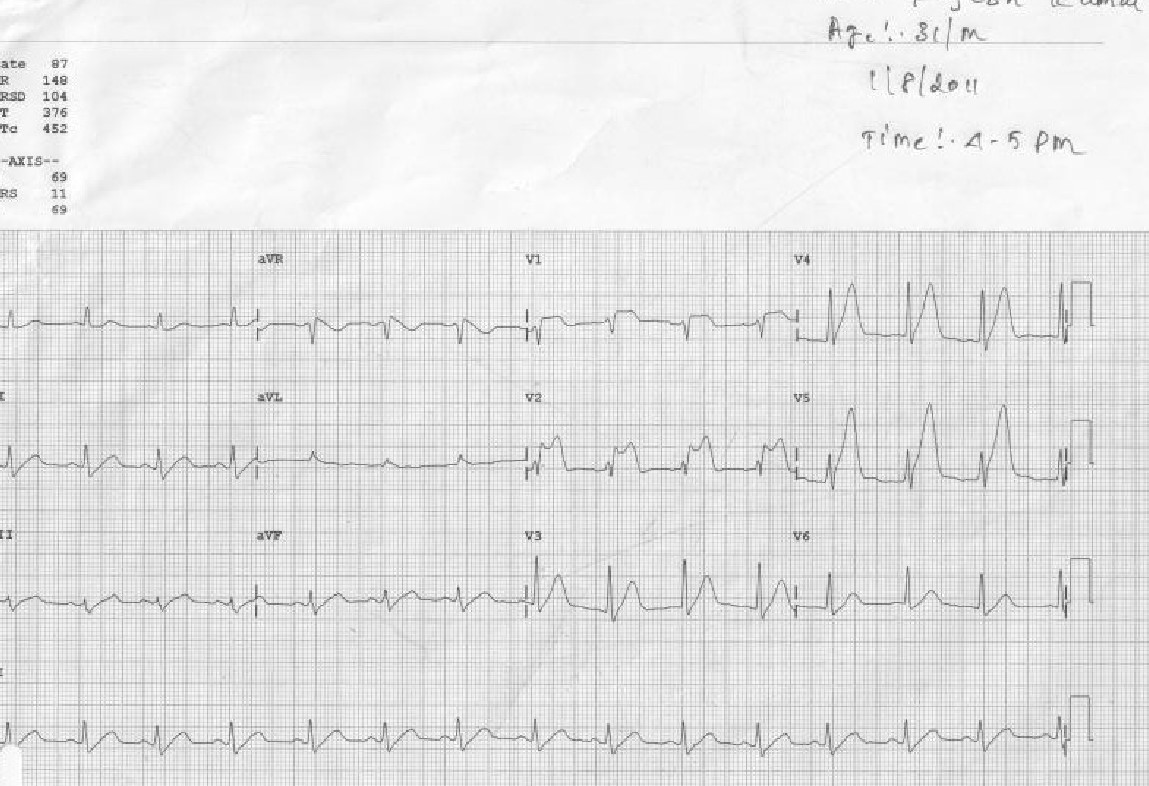
The treatment was Initiated in 10 minutes and completed in an hour, (Those days cath lab wasn’t functioning 24/7, more importantly, there was no external interference with our professional decision-making process)
The ECG was repeated at 7.15 PM
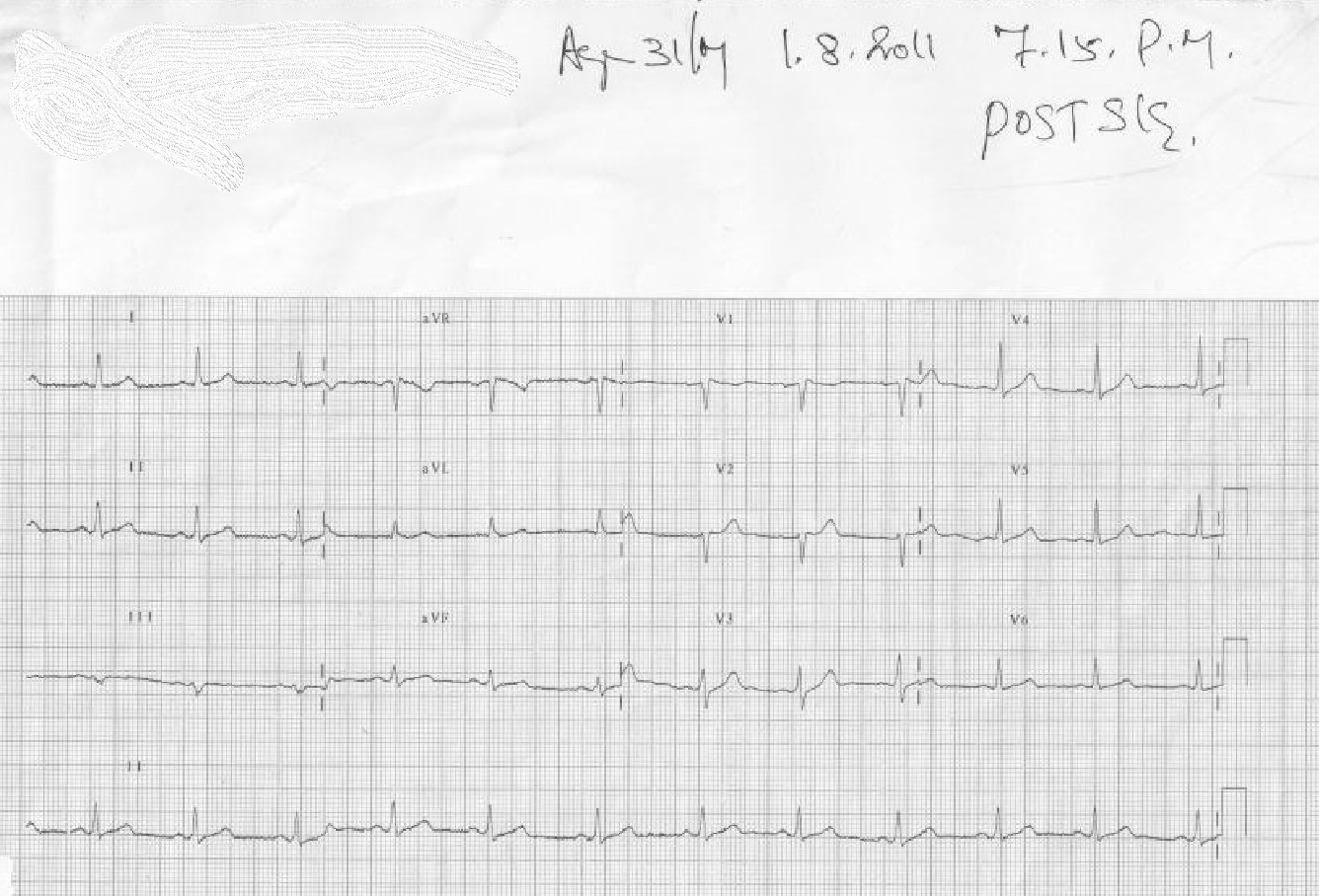
I think this case is much relevant even today, because it made me guilty of committing a crime*, by treating a STEMI without the help of a cath lab and discharging the patient with near normal ECG and LV function. The guilt was further amplified as I had used the lowly streptokinase, and not the glamorous Tenecteplase which could have produced a brisker and more complete TIMI 3 flow.
*One of my corporate friend called it a heinous one by current standards, for not attempting to visuvalise the IRA and a possible pharmaco invasive PCI.
Final message
STEMI can be tackled successfully in a number of different strategies. Immediate cath lab care is an optional accessory in the majority and of course, it can be life-saving in the minority. If we are unable to differentiate which patient will truly benefit from urgent cath lab intervention, I think, we have a huge problem, with the way we learn and teach cardiology. Hiding behind double-blinded statistics and RCTs is not going to bring a solution to this largely self-inflicted scientific predicament;



