Here is a brand new study on Digoxin from AIIMS-India , in 2026 that triggered this post. (Ref 2)
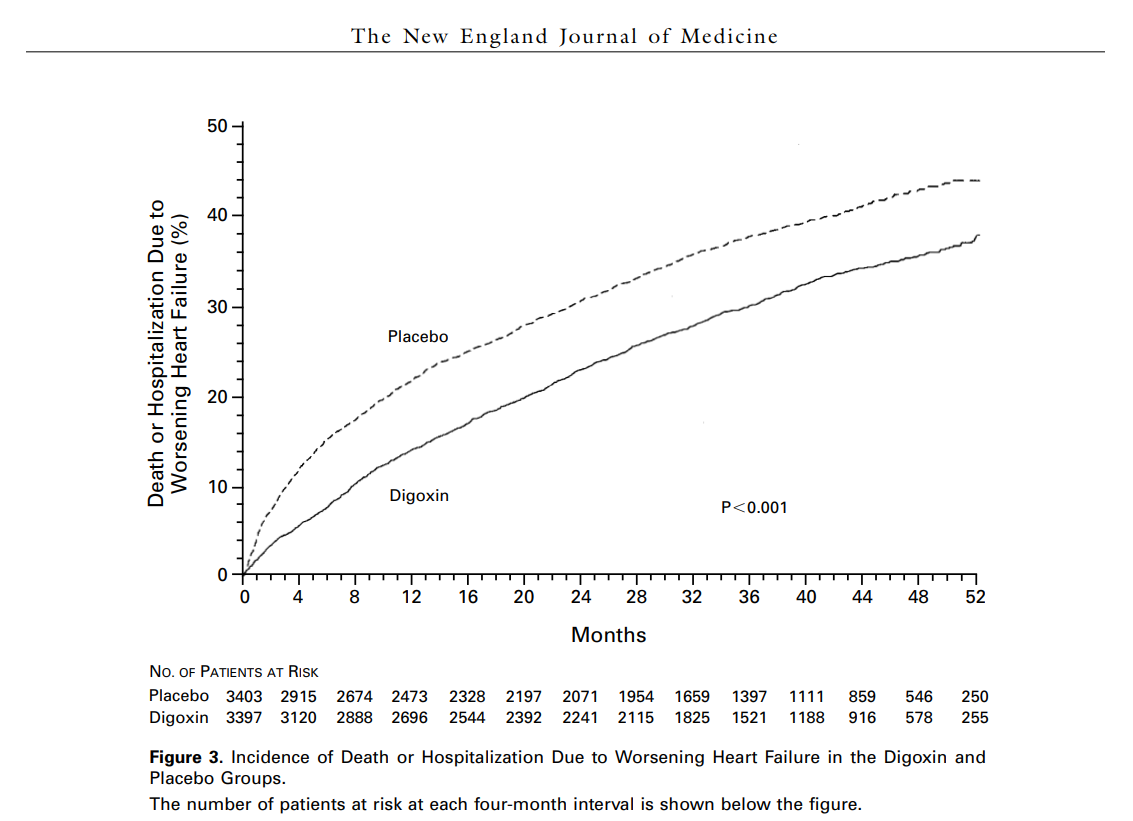
The DIG trial published more than 3 decades ago,(1997) was a landmark study, that applied a disruptive break on the widespread usage of digoxin in heart failure for all the wrong reasons. It is one of the good examples of , how badly the mainstream academia could interpret a study. Though the study showed a consistent reduction in worsening heart failure and hospitalization, yet no overall mortality benefit was accrued in the full trial population. This apparent paradox deserves a more careful interpretation. We need to ask one simple question.
Did the DIG trial reported how many acute deaths (In hospital) occurred among patients who were on digoxin and who weren’t ?
The answer is No. While the paper details how many patients were hospitalized and how many died of heart failure, it does not specify which of those heart failure deaths happened specifically while the patient was admitted in- hospital. Then, DIG trial also played the same old game of all major RCTs. Death and worsening heart failure was clubbed as a combined end point, for analysis. So, we don’t know the exact acute deaths, that were prevented by Digoxin. Why no one asked this question for so long ?
Did we mis-understand the DIG-Trial ?
Further, it is plausible Digoxin’s life-saving role probably lies in preventing the decompensated episode itself.
Of course, patients ( Who were non on digoxin)may still survive because modern therapy , with powerful diuretics, ventilation, inotropes, and intensive care .Still, we know there is a specific (could be high ) mortality rate in all acute decompensated heart failure cases despite the best treatment. The statistics ignored those lives that were lost due to decompensation , because of non-administration of digoxin.
Modified version of for DIG-Trial conclusion
“Digoxin may save lives by reducing the frequency and severity of decompensated heart-failure episodes, thereby preventing some acute deaths and the need for ICU care. However, DIG trial failed to show an overall mortality benefit in the study population in long term. This is understandable, as heart failure is a progressive disease.”
Final message
It doesn’t make sense to make a blanket statement that Digoxin doesn’t prevent deaths in heart failure. However huge/ popular a study may be, it need to undergo scrutiny beyond evidence and statistics. How ? They should be subjected to the vigorous test of bedside trial on individual patient* , common sense and experience.(* Recall N-1 study Ref 4)
Reference
We are gathering more evidence in favor of Digoxin in recent times.



