Archive for the ‘Uncategorized’ Category
A shared “Judicial & Medical” quote
Posted in Uncategorized, tagged humanity in medicine, medcial ethics, science and medicine on December 24, 2025|
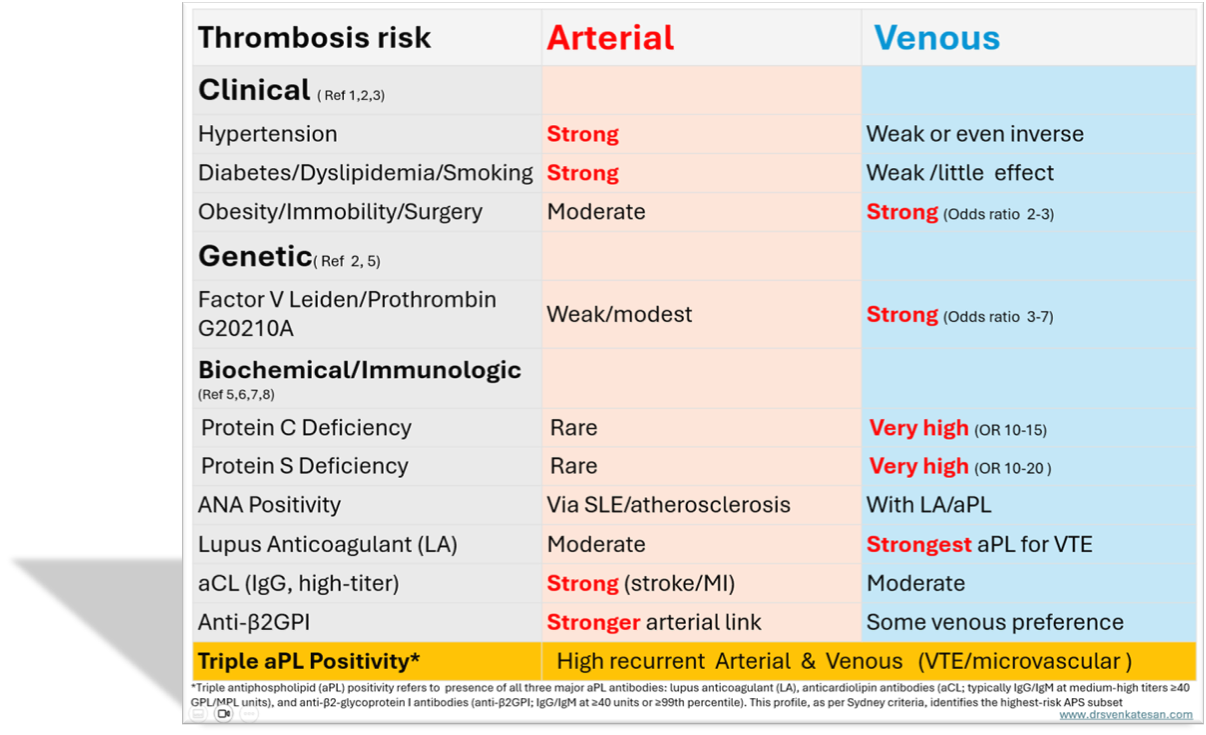
Pro-coagulant state: Arterial vs venous thrombus risk , what are the differences ?
Posted in Uncategorized on December 21, 2025|
It would be silly to remind, it’s the same five liters of blood, that circulates across, both the arterial and venous system. But, its journey one away from the heart, and the other towards the heart are strikingly different. They are subjected to various hemodynamic forces, travels different terrains, at different speeds, thousands of kilometers of microvasculature along the cardiovascular highway, yet merging with each other every 15 seconds or so, at the pulmonary junction box. Have a look at the following images, to understand the distribution of the blood volume.


The first image is taken from the maverick physiologist Dr. Guyton’s textbook of physiology, and the second one from the equally famous Dr. Ganong’s. Both images depict the distribution of blood volume, the corresponding pressures, and velocity. Every cardiology fellow should recall these two images even in their sleep. Also mind, they circulate around the body, lifelong without clotting or bleeding, assisted by the right balance of pro and antithrombotic forces.
Why some of patient’s blood is more likely to get frozen ?
Logic would suggest venous thrombosis should be more prevalent than arterial thrombosis at any point of time and location. This is due to the slowness of the circulation and the enormous volume within the venous reservoir. But is this the clinical reality? It is indeed true, that incidence of minor venous thrombosis exceeds arterial thrombosis. Since venous thrombosis often gets lysed or get stuck in the lungs, it’s frequently under-recognized. Arterial thrombosis causes more damage in an important sense, as it leads to target organ ischemia.
Apart from hemodynamic factors, the 200 year old Virchow’s triad is very much alive. The vessel wall integrity, intrinsic defects in the coagulation and anticoagulant/fibrinolytic molecules, the genetic susceptibility are the important determining factors. The RBC and platelet behaviour too changes, in high and low pressure environments.
How to diagnose a patient who is in a procoagulant state?
The topic is so complex .Many things are still poorly understood. We should have a checklist of all systemic conditions that can cause increased risk of thrombus. We know pregnancy is inherently a procoagulant state, as is manifest or concealed malignancy.
What we normally do ?
It is very easy to tick the coagulation profile/panel slip and pass it on to the nursing staff. Some of us take another easy route, referring such patients to a rheumatologist for the risk-stratifying job. This is probably because we strongly believe SLE and connective tissue disorders are the first culprits.
I think we need to engage the hematologist more often because thrombosis is not only due to excess coagulation. It is also due to a lack of enough circulating anticoagulants. (As a cardiologist, sometimes I feel awkward. to call myself an expert of the circulatory system, with almost zero knowledge of how the blood clots or dissolves.) This article tries to differentiate the risk factors operative on the venous and arterial sides. It is only a gross attempt; many risk factors are invisible and are common between arterial and venous thrombus.
For a detailed analysis of Sydney criteria /ACR-EULAR (Reference 7 )
How to treat pro-coagulant state?
Fortunately, identifying the thrombosis prone patients is complex , but the treatment is fairly simple. We have only few options: Aspirin, Warfarin, and NOACs *We need to choose one of them. The general rule is aspirin doesn’t work much on the venous side. I don’t know how far this is really true. (It has something to do with the shearing force of platelets? ) However, in obstetrics, the placental circulation is full of low pressure venous plexus where Aspirin is used as a norm.
Between Warfarin and NOACs, there is absolutely no doubt Warfarin is the clear winner on the arterial side. Because of monitoring issues and fear of bleeding, we are compelled to switch to NOACs in many situations. Beware, think twice before prescribing NOAC for prophylaxis against arterial thrombus. The venous side does not have much difference in choice. *Heparin (& its glamor sibling LMWH) is a unique molecule, which has ability to work on both arterial and venous sides.
References
Postamble
The article doesn’t discuss the intra vascular metals, wires, devices, valves, pacemakers , related thrombosis. Here there is a known trigger. It is possible, they also influenced by the baseline factors of pro-coagulation discussed above.
“Stand alone thrombolysis’ can reign in STEMI in majority, unless we wish to,pull it down !
Posted in Uncategorized on December 15, 2025|
“When we change the way we look at things, the things we look at change.”
Wayne Dyer
Standalone thrombolysis remains a potent, evidence-based, time tested lifeline for STEMI patients worldwide.It delivers rapid myocardial salvage. This is a rule,not an exception ,where primary PCI delays or pharmaco-invasive infrastructure falter, with absolute mortality reductions of 2-3% when administered early . The benefits holds on or often beats pPCI despite it’s relative edge in ideal settings.
STEMI : Time trumps technology
Fibrinolysis, as a modality has pioneered the science of myocardial reperfusion. It reduced the early mortality by >50% in landmark trials enrolling tens of thousands, and still stands tall. it carries (Class I-A Indication ) Pharmaco-invasive strategies reduce reinfarction by 2% absolute (NNT 50) over lysis-alone but show only uncertain 0.5% mortality gains (NNT -200, low-certainty), as per the 2025 PLOS ONE meta-analysis of 7 RCTs .
This is major evidence stress an important hidden truth , that standalone lysis is not “obsolete” in low-risk, well-reperfused cases where PCI risks (bleeding, microvascular injury) may offset slim benefits.(Soriano-Moreno DR 2025 PLOS ONE meta analysis)
Real-world registries confirm this. In >70% of global STEMI (LMICs, rural/high-transfer areas), lysis achieves TIMI 3 flow in 50-60% and can beat the delayed PCI prognostically., if door-to-needle <30 minutes . More importantly (& not so-scientifically too) TIMI 2 flows are not considered as success in most of these studies. In reality, an early TIMI 2 flow, which can be achieved with lytics easily, is more than good enough to prevent myocardial necrosis. This is in contrast to the fact, that even a glorious TIMI 3 flow, after PCI does not guarantee complete myocardial reperfusion.
Systems reality: Equity vs PCI hegemony
Population-based registries indicate primary PCI utilization rates below 20% for STEMI cases in India, or other developing countires.
Compulsive mandates, that prioritise PCI, increase total ischemic time, elevate no-reflow incidence, and raise mortality compared to systems enabling universal early fibrinolysis. The most troubling truth is, non-PCI centers hesitate to deliver timely fibrinolysis , due to perceived Inferiority, peer pressure , potentially forgoing established mortality benefits.
Commercial undercurrents: Incentives could Injure the myocardium
PCI ecosystem prioritizes procedural volume metrics, cardiologist’s Incentives, reimbursements (10-20 times higher than fibrinolysis costs), and institutional performance indicators, resulting in under-investment in fibrinolysis infrastructure. This systemic bias potentially compromising overall STEMI outcomes by deprioritizing rapid reperfusion strategies.
Final message
Cardiology Literature Needs a Scientific Distillation & a Philosophical Kick
Modern cardiology’s PCI dogma is trying to blind thrombolysis’s enduring truth. A village PHC’s or ER crew’s humble hand injections at 30 minutes could salvage more myocardium than a helicopter transferred PCI, in a star rated cathlab.
Standalone lysis fights STEMI fiercely, early, equitably, economically, unless commercial narratives, transfer dogma, and selective trials confer them a cult status, exposing millions of ACS patients to prolonged ischemia.
Are we reqdy to revive and embrace the truth? Population-based pPCI can wait. It is a futile to set wrong goals like “stent for every STEMI”; not only in a country like India, it applies to even the developed nations. Let us, prioritize lysis-first systems, especially the pre-hospital or ultra-fast in-hospital lysis. Reserve pharmaco-invasive PCI for failures or high-risk, especially with built in harm seen with routine early PCI post-lysis.
References
- Bouyaddid S, Bouchlarhem A, Bazid Z, Ismaili N, El Ouafi N. Pharmaco-invasive Therapy: A Continued Role for Fibrinolysis in the Primary PCI era. Clin Appl Thromb Hemost. 2023;29:10760296231221549. doi:10.1177/10760296231221549. https://pubmed.ncbi.nlm.nih.gov/38145624/pmc.ncbi.nlm.nih
- Armstrong PW, Gershlick AH, Goldstein P, et al. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2013;368(15):1379-1387. doi:10.1056/NEJMoa1304062. https://www.nejm.org/doi/full/10.1056/NEJMoa1304062ncbi.nlm.nih
- Assessment of the Safety and Efficacy of a New Thrombolytic Regimen (ASSENT)-4 PCI investigators. Primary versus tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction (ASSENT-4 PCI): randomised trial. Lancet. 2006;367(9510):569-578. doi:10.1016/S0140-6736(06)68148-0. https://pubmed.ncbi.nlm.nih.gov/16488800/pubmed.ncbi.nlm.nih
- McDonald MA, Fu Y, Zeymer U, et al. Adverse outcomes in fibrinolytic-based facilitated percutaneous coronary intervention: insights from the ASSENT-4 PCI electrocardiographic substudy. Eur Heart J. 2008;29(7):871-879. doi:10.1093/eurheartj/ehm599. https://academic.oup.com/eurheartj/article/29/7/871/483738academic.oup
- Pinto DS, Kirtane AJ, Ruocco TA Jr, et al. Facilitated percutaneous coronary intervention following fibrinolysis: the path to redemption? Insights from BRAVE, GRACIA, and beyond. Rev Cardiovasc Med. 2007;8(4):187-194. https://pubmed.ncbi.nlm.nih.gov/18192961/pmc.ncbi.nlm.nih
- Steg PG, James SK, Atar D, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33(20):2569-2619. doi:10.1093/eurheartj/ehs215. https://academic.oup.com/eurheartj/article/33/20/2569/4095042academic.oup
- Soriano-Moreno DR, Tuco KG, Delgado Flores CJ, Flores-Lovon K, Ccami-Bernal F, Quijano-Escate R, López-Rojas LM, Goicochea-Lugo S. Pharmacoinvasive strategy versus fibrinolytic therapy alone in adults with ST-elevation myocardial infarction: A systematic review and meta-analysis. PLoS One. 2025 Oct 9;20(10):e0334309. doi: 10.1371/journal.pone.0334309. PMID: 41066493; PMCID: PMC12510495.
Looking beyond TIMI 3 flow : Redefining True Success in pPCI
Posted in Uncategorized on December 12, 2025|
This is an editorial submitted by this author to a leading cardiology journal, which was returned within 24 hours , with a comment that article is unsuitable for publication .Want to know, whether the readers agree with the journal editorial team
The Unfinished Story of “Successful” Primary PCI
Primary percutaneous coronary intervention (pPCI) has revolutionized the management of ST-elevation myocardial infarction (STEMI) and remains the gold standard for restoring coronary perfusion. Angiographic success defined as achieving Thrombolysis in Myocardial Infarction (TIMI) grade 3 flow in the infarct-related artery occurs in more than 90–95% of cases. (1,3)However, this measure reflects epicardial recanalization alone and falls short as an indicator of effective myocardial reperfusion..(5)
Cardiac magnetic resonance (MRI/CMR) imaging, myocardial contrast echocardiography, and nuclear perfusion techniques consistently reveal that adequate tissue-level reperfusion occurs in only 60–70% of patients with angiographically successful PPCI. This disparity highlights a critical gap between procedural endpoints and true myocardial salvage.(6)
The Persistent Challenge of Microvascular Obstruction
Despite apparent angiographic success, up to 20–30% of patients exhibit microvascular obstruction (MVO) or “no-reflow.” The pathophysiology of MVO involves distal microembolization, capillary edema, and endothelial dysfunction. (2)
MRI studies have demonstrated MVO in 10–15% of PPCI-treated patients with TIMI 3 flow, often associated with larger infarct size, lower left ventricular (LV) ejection fraction, and worse long-term outcomes. (4,6)
Redefining the Endpoints: From Epicardial Patency to Microvascular Integrity
Left ventricular function remains the most clinically relevant indicator of therapeutic success in STEMI. Persistent LV dysfunction in up to 40% of successfully revascularized patients underscores the inadequacy of angiography based assessment. (3)
TIMI grading system is the universally adopted most popular angiographic flow grading. It has its limitations . It confines with epicardial flow . The max grade is TIMI 3 , and it sort of falsely reassures
The concept of TIMI 4 flow was originally suggested by Dr Gibson in 1999 , calling hyperemic flow with a low TIMI fame count, as TIMI 4 flow. For some reason this concept was never adopted, though this term extends the traditional TIMI grading system to include microcirculatory perfusion.
This proposed category reflects optimal tissue level reperfusion, measurable through myocardial blush grade, the index of microcirculatory resistance (IMR), or perfusion-based MRI parameters. (8,10)TIMI 4, therefore, would define the ultimate therapeutic endpoint in the physiological perfusion at the myocyte level.
Emerging Tools and Strategies for Microvascular Optimization
Several strategies can favorably influence microvascular flow. Intracoronary vasodilators such as adenosine, verapamil, and sodium nitroprusside mitigate microvascular constriction and distal embolization. Deferred stenting techniques may reduce reperfusion injury in selected cases.
Recalibrating the Definition of Successful pPCI
Given the growing evidence base, it is time to reconsider what constitutes “success” in pPCI. A restored epicardial lumen without adequate tissue perfusion represents an incomplete therapeutic achievement.
A Call to Global Cardiovascular Leadership
It is good, if the major professional societies like the American College of Cardiology (ACC), European Society of Cardiology (ESC), and Society for Cardiovascular Angiography and Interventions (SCAI) reassess the criteria used to define procedural success in STEMI interventions. Integrating TIMI 4 flow as a recognized endpoint, along with preservation of maximal left ventricular function, will more accurately define the true success of pPCI.
References
- Sarkar A, Shravage P. TIMI Grade Flow. https://www.ncbi.nlm.nih.gov/books/NBK482412/ncbi.nlm.nih
- Wu KC. CMR of microvascular obstruction and hemorrhage in myocardial infarction. J Cardiovasc Magn Reson. 2012 Nov 22;14:68. ttps://pmc.ncbi.nlm.nih.gov/articles/PMC3514126/pmc.ncbi.nlm.nih
- Henriques JP, et al. Predictors of suboptimal TIMI flow after primary angioplasty for acute myocardial infarction: insights from the ATLANTIC trial. EuroIntervention. 2024 Jun 17. https://eurointervention.pcronline.com/article/predictors-of-suboptimal-timi-flow-after-primary-angioplasty-for-acute-myocardialeurointervention.pcronline
- Jeyaprakash P, et al. Index of Microcirculatory Resistance to predict microvascular obstruction in STEMI: a meta-analysis. Catheter Cardiovasc Interv. 2024 Feb. https://pubmed.ncbi.nlm.nih.gov/38179600/pubmed.ncbi.nlm.nih
- Zeymer U, et al. Impact of TIMI 3 patency before primary percutaneous intervention on outcome in patients with STEMI. EuroIntervention. 2012 Aug;8(8):900-7. https://pmc.ncbi.nlm.nih.gov/articles/PMC3760529/pmc.ncbi.nlm.nih
- Eitel I, et al. Clinical Impact of Persistent Microvascular Obstruction in CMR After Reperfused STEMI. JACC Cardiovasc Imaging. 2025. https://pubmed.ncbi.nlm.nih.gov/40357554/pubmed.ncbi.nlm.nih
- Pantea-Roșan LR, et al. No-Reflow after PPCI—A Predictor of Short-Term Mortality in STEMI. J Clin Med. 2020 Oct 8;9(10):3145. https://pmc.ncbi.nlm.nih.gov/articles/PMC7563881/pmc.ncbi.nlm.nih
- Fearon WF, et al. One-year results from the Assessing MICRO-vascular resistances via IMR to predict outcome in ST-elevation myocardial infarction patients with multivessel disease undergoing primary PCI (AMICRO) trial. Front Cardiovasc Med. 2022 Dec 1;9:1051174. https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2022.1051174/fullfrontiersin
- de Waha S, et al. Prognostic Value of Myocardial Blush Grade in ST-elevation MI. J Am Coll Cardiol. 2022. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9340576/pmc.ncbi.nlm.nih
- van ‘t Hof AW, et al. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Circulation. 2001 Aug 28;104(9):1130-4. https://pmc.ncbi.nlm.nih.gov/articles/PMC2810032/pmc.ncbi.nlm.nih
How to select a wrong patient for PCI, in stable multi vessel CAD ?
Posted in Uncategorized on December 12, 2025|
Revascularization in chronic CAD is be primarily based on
A. Angina & its severity
B. Inducible Ischemia by stress test
C. Coronary anatomy & FFR/IFR based.
D.Total Plaque burden , plaque morphology & Vulnerability
E.As per the cardiologist’s wish
F As per patient’s wish or their Insurance limits
Trying to Answer
*Revascularization means, first we should document, there is significantly reduced baseline myocardial blood flow to the distal myocardium (which would mean near total block).
*Then, we must realize ischemia and angina are two different things. Ischemia can exist without angina; similarly, angina can occur without an obstructive epicardial lesion, that is due to demand or microvascular disease.
*It is also vital to understand that PCI or CABG is meant mainly for symptom relief. PCI is just a lesion-specific temporary fix. Note that symptom means angina; dyspnea relief after revascularization, either by PCI or CABG, is an exception, not a rule.
*Plaque burden and its vulnerability are major determinants of long-term survival. In multivessel CAD, we can’t attend to all by PCI.
*It is also a fact that , while PCI can successfully fix an eccentric vulnerable plaque, it can very easily destabilize a non-vulnerable plaque if the metals are not maintained properly.
*It is wise to understand medical management , which by stabilizing and regressing a plaque, is technically a medical revascularization process . I am sure no cardiologist would be ready to accept this (Request them to go through AVERT study : Atorvastatin beats PTCA) So, the correct decision to revascularize is based on the presence of significant symptoms of angina that are refractory to a trial of anti-anginal drugs.
Reference
Few are worth mentioning* (As RCTs seem to fight with each other)
*There are dozens of guidelines and hundreds of RCTs, and meta-analyses that have addressed this question. I am afraid none have answered it clearly or we are not able to follow it, as the conclusions colludes with our wish. Not being able to find an answer to research question despite large systematic studies, implies, RCTs may not be the real solution in many clinical queries.
Hardware update : Ringer coronary perfusion catheter for perforation management.
Posted in Uncategorized on December 10, 2025|
Coronary arterial perforation continues to be challenging task . There are multiple options to arrest the perforation as listed below.
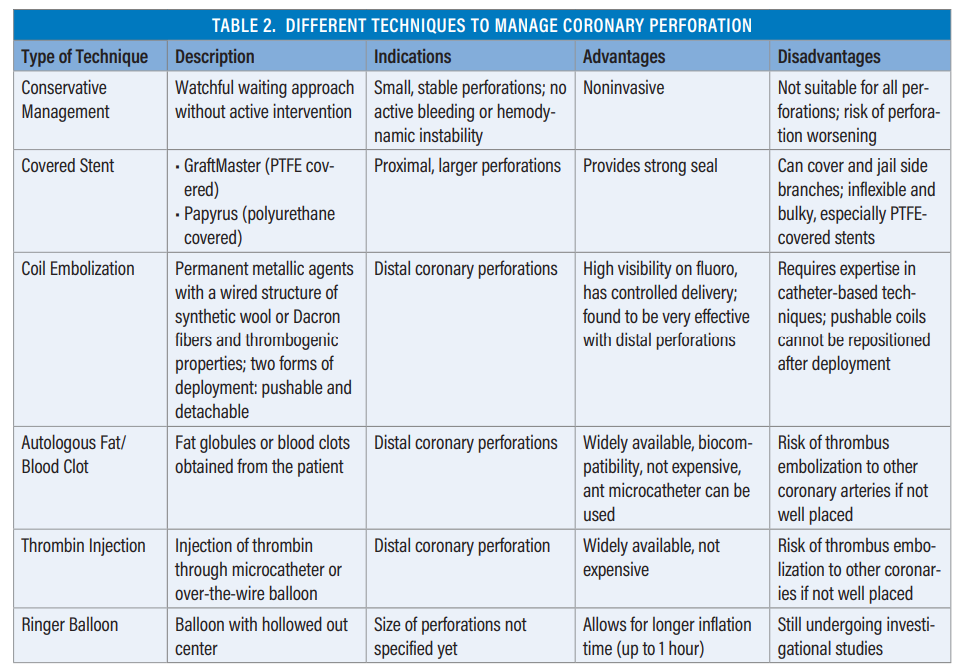
Image source Ref : 1
Still, we don’t have a quick balloon occlusion strategy that maintains antegrade flow. Here is a new innovation, a circumferentially inflating balloon (like an airbag or a parachute from the catheter) that can maintain the antegrade flow. This may be vital in salvaging or preventing a myocardial infarction. This balloon catheter is named the Ringer balloon, manufactured by Teleflex. ( _K_andzari DE, Alqarqaz M, Nicholson. et al J Soc Cardiovasc Angiogr Interv.2025 Jul 22;4(7):103575. doi: 10.1016/j.jscai.2025. )
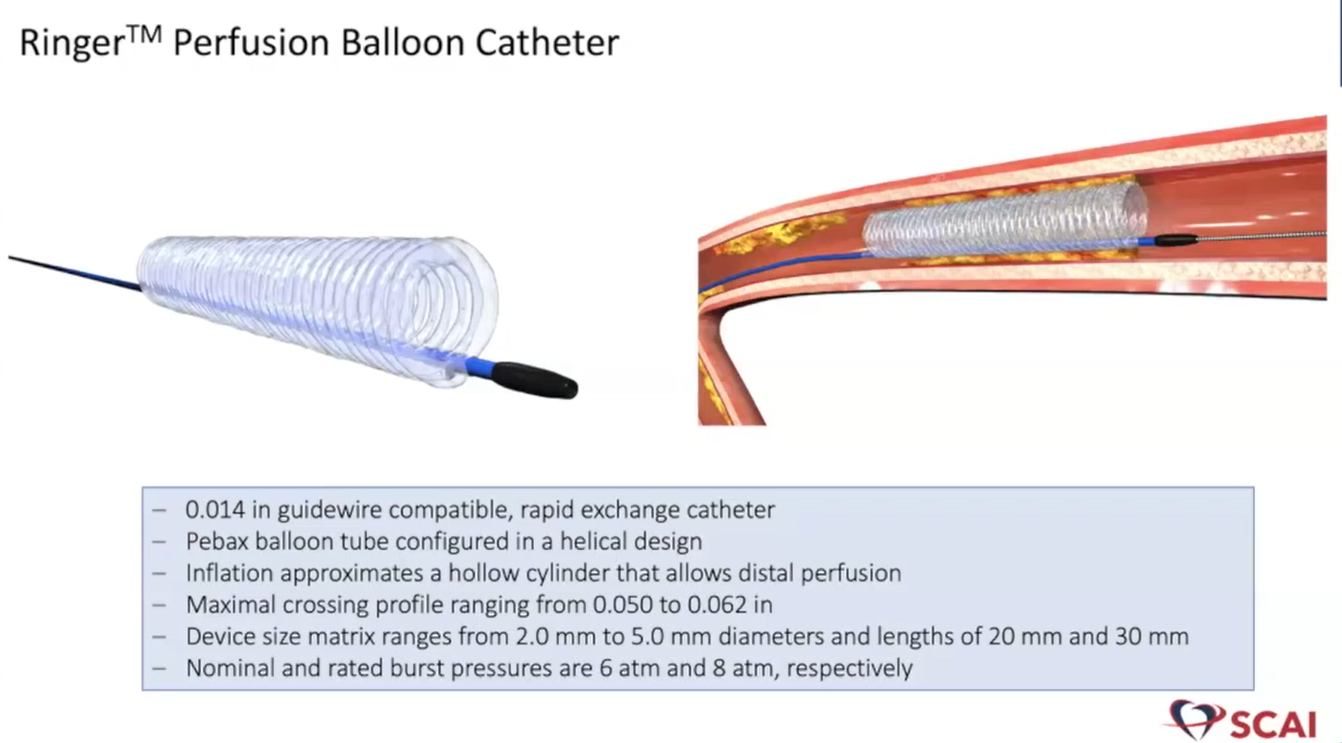
Source : Teleflex website
Reference
1.Perforation-management ,A review article Molly Silkowski, Anbukarasi Maran, -An assessment of balloon tamponade, Ringer balloon, covered stents, coils, and thrombin.
2.Link to the Teleflex website
AI clinical consults : Beware of machine hallucinations, that could become a permanent medical record of your patients.
Posted in Uncategorized, tagged AI assitted consultation in hospitals, AI consultations, AI in medical profession, ai in medicine, annals of internal medicine, Artificial Intelligence in cardiology, bmj, jama network, journal of AI in medicine, lancet, nejm on December 6, 2025|
It is predicted, (or already happening ) atleast 30 % of clinical consults happen with AI assistsnce or with completely with machines.

The Initial work up is suggested by the AI bots, even in ER rooms. They may be right in 80% of times. But, who is it to filter and grab those remaining 20%. No one , except a astutely learnt clinician. Unfortunately, there is no super AI to do this job.
Final message
This is the beginning of, a new exciting & dangerous era, for the medical profession. If we are not vigilant or loose our common sense, these bots will soon reach their next destination, ie patient’s bed side.
Reference
BMJ in its current Issue address these aspects of increasing AI usage in the clinical consults
1. Clinical competencies for using generative AI in patient care BMJ 2025; 391 doi: https://doi.org/10.1136/bmj-2025-085324
Guilty lessons in cardiology : Learn to Ignore significant LV dysfunction, following a successful primary PCI
Posted in Uncategorized on December 4, 2025|
Interventional cardiology’s flag-bearing procedure primary PCI stands tall and is being projected to be the greatest thing to happen for the human heart during the critical times of STEMI. The aim is to do a fast PCI to salvage the myocardium. Unfortunately ,It has become a strange habit, (endorsed by even learned cardiology forums) to define the success of primary PCI based on the restoration of TIMI 3 flow in the IRA, and not on the amount of myocardium salvaged .
What is more worrisome is, the fact, that almost every experienced cardiologist knows, crystal clear, that there is a pitiful relationship between TIMI flows at the epicardial artery and subsequent LV function. Of course, it might improve as time goes on. Still, it is unacceptable to define success of pPCI prematurely. some times, as early as the patient is wheeled out of cath lab.
What does the evidence say ?
The incidence of moderate or severe LV dysfunction even after a timely pPCI is still significant. The average incidence hovers around 36% .It would mean , atleast one third of patients who undergo pPCI leave the hospital with significant myocardial damage, but the cath lab report would say proudly , it is a successful pPCI without any untoward events. (Mind you, in the strict sense, even treated no-reflow should come under partial failure of pPCI, which again constitutes another 20%) Ref : Papapostolou S, et al, A Long-term clinical outcomes of transient and persistent no-reflow following percutaneous coronary intervention (PCI): a multicentre Australian registry. EuroIntervention. 2018 Jun 20;14(2):185-193.
Comparative studies that looked into LV function following pPCI
| Study (Year, Location) | Sample Size | LV Dysfunction Definition | Incidence (%) | Key Predictors |
|---|---|---|---|---|
| Khaled et al. (2022, Saudi Arabia) | 2863 | LVEF ≤30% (early, <24h echo) | 36% | Anterior STEMI, high troponin, renal impairment, multi-vessel disease |
| Liu et al. (2023, China) | 186 | LVEF decline (long-term, 4y) | 54 % | High peak troponin I, anterior STEMI, prior MI, low baseline LVEF |
| Kim et al. (2018, Korea) | 1736 | LVEF ≤40% (3-12m echo) | 14% | Baseline LVEF ≤40%, renal insufficiency, high peak CK/CKMB |
| Parodi et al. (2007, Italy) | 500 | <40% (Variable) | 27-60% range cited | Anterior MI, large infarct size |
| HORIZONS-AMI (2011) | Large RCT | Heart failure post-PCI | 5-9% | Thrombus burden, delayed reperfusion |
Note a curious point : The HORIZONS-AMI had a very low incidence of LV dysfunction totally a disconnected with the reality
Final message
It is a height of deceit, when some of us are still canvasing patients, emphasizing , that it has 95% success, hiding behind the TIMI 3 flow at IRA. Still waiting for the day of reckoning (Read my 2016 presentation in CSI Kochi conference) when the ACC/ESC/SCAI , will ultimately redefine the definition of successful pPCI to include a cut off of post-procedure EF of at least 50%.
Let us not stop with that, we have to mitigate the LV dysfunction with all our might. This implies early preventive and protective measures to maintsin the microvascular integrity , which is responsible for this epicardial-myocardial dissociation.
Reference
- Khaled S, Shalaby G. Severe left ventricular dysfunction earlier after acute myocardial infarction treated with primary percutaneous coronary intervention: predictors and in-hospital outcome. A Middle Eastern tertiary center experience. J Saudi Heart Assoc. 2022;34(4):257-63. https://doi.org/10.37616/2212-5043.1325sha257-263.pdfj-saudi-heart
- Liu C, Guo M, Cui Y, Wu M, Chen H. Incidence and predictors of left ventricular function change following ST-segment elevation myocardial infarction. Front Cardiovasc Med. 2023;10:1079647. https://doi.org/10.3389/fcvm.2023.1079647pmc.ncbi.nlm.nih+1
- Kim DH, Park CB, Jin ES, Hwang HJ, Sohn IS, Cho JM, Kim CJ. Predictors of decreased left ventricular function subsequent to follow-up echocardiography after percutaneous coronary intervention following acute ST-elevation myocardial infarction. Exp Ther Med. 2018;15(5):4089-96. https://doi.org/10.3892/etm.2018.5962spandidos-publications+1
- Parodi G, Memisha G, Carrabba N, Signorini U, Migliorini A, Cerisano G, Bolognese L. Prevalence, predictors, time course, and long-term clinical implications of left ventricular functional recovery after mechanical reperfusion for acute myocardial infarction. Am J Cardiol. 2007;100(12):1718-22. https://doi.org/10.1016/j.amjcard.2007.07.022pubmed.ncbi.nlm.nih
- Kelly DJ, Gershlick T, Witzenbichler B, Guagliumi G, Fahy M, Dangas G, Lansky AJ, Mehran R, Stone GW; HORIZONS-AMI Trial Investigators. Incidence and predictors of heart failure following percutaneous coronary intervention in ST-segment elevation myocardial infarction: the HORIZONS-AMI trial. Am Heart J. 2011;162(4):663-70. https://doi.org/10.1016/j.ahj.2011.07.032pubmed.ncbi.nlm.nih+1
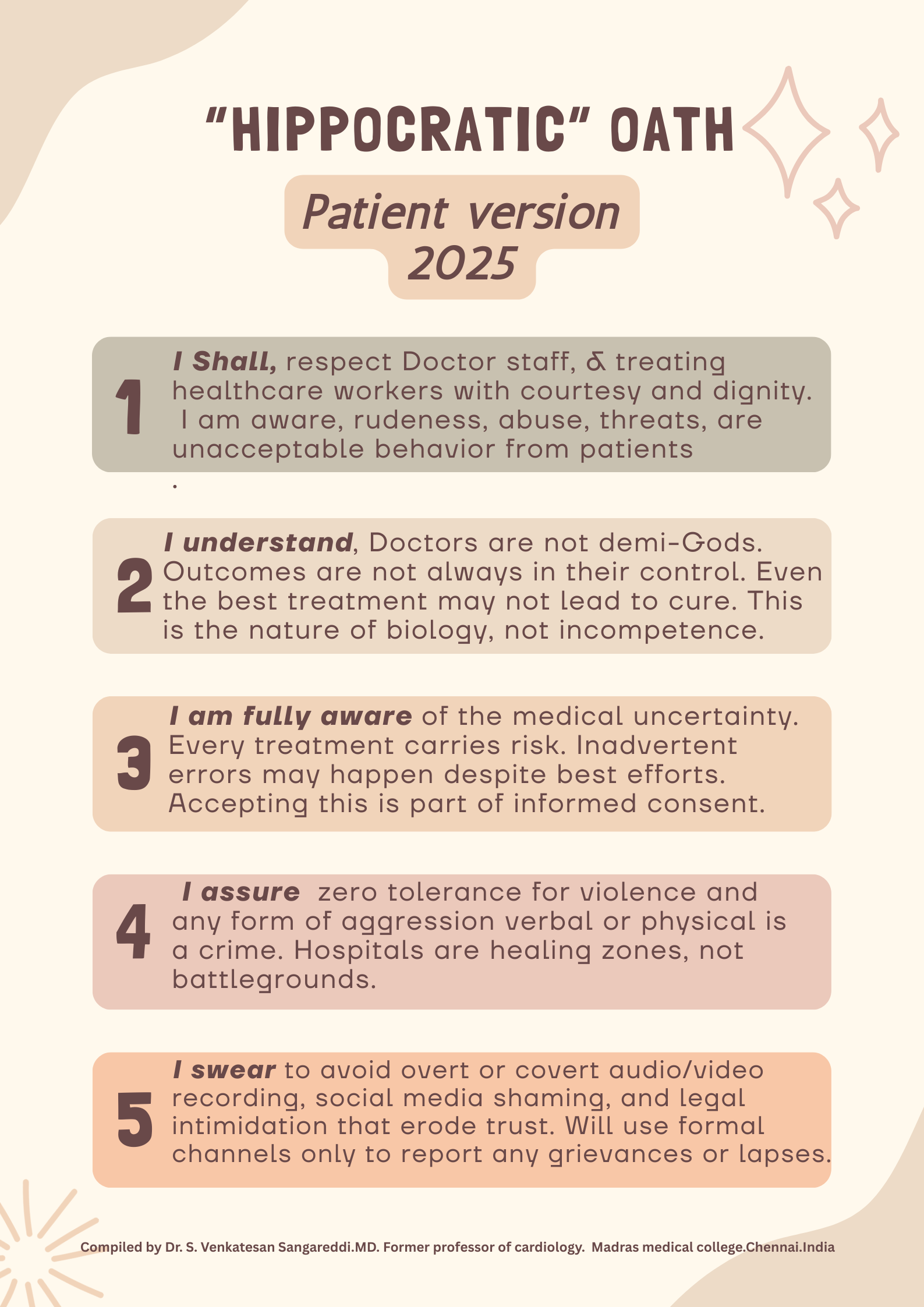
Hippocratic oath : A Patient version
Posted in Uncategorized, tagged hipocratic path patinet version, Hippocratic oath, medcial education, medcial ethics on December 4, 2025|
While patient rights has been extensively discussed and debated , there is some concern especially in country like India, where violence against medical professionals has increased to prohibitive levels. This is mainly attributed to low levels of tolerance and high expectations from the doctors and hospitals.
There has been multiple Incidents where doctors are attacked, even when a life is lost due an incurable disease in spite of well administered treatment . Many patients are unable to differentiate the natural history of illness , any death is looked upon as medical negligence. In this context, there is a call for patient education and teaching them responsibilities and make them understand the complexity and uncertainty in the science of biology, and also accept the reality of inadvertent errors in judgment and execution in medical practice.
A curious solution is suggested .Yes , its called Hippocratic Oath : Patient version .The father of medicine would have never thought , a day would come , when patients might, try to prevail over the Doctors .Readers may decide about the political correctness , utility and practicality of such an oath.

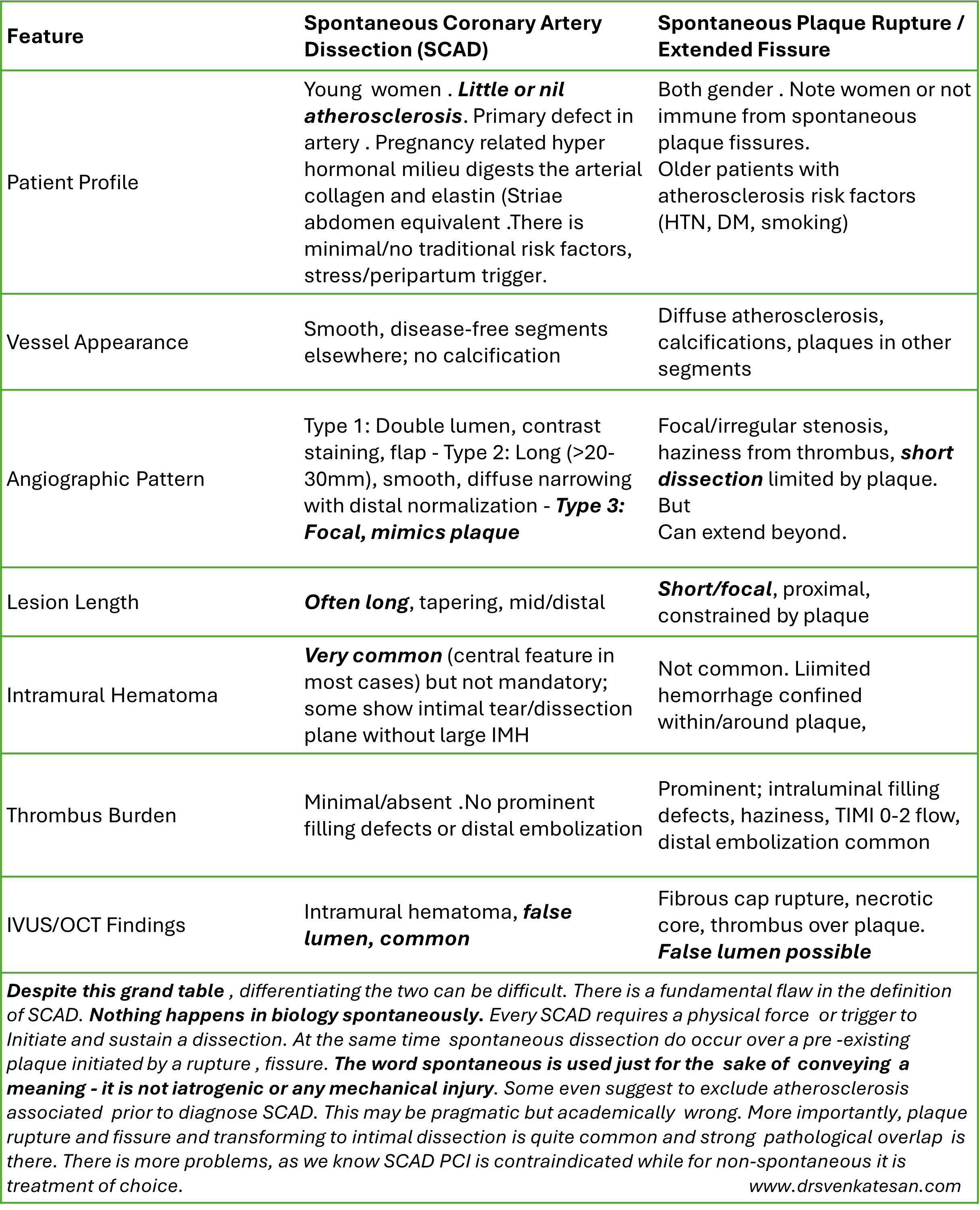
SCAD : No dissection is spontaneous
Posted in Uncategorized on December 2, 2025|
“Nothing moves without an external physical force”
SCAD is a popular entity among cardiologists in angiographically sub-categorizing of ACS, especially in women. The entity is indeed important to recognize, as the otherwise omnipresent PCI, is contraindicated in SCAD.
Meanwhile, we can’t take every suspicious-looking dissecting flap as SCAD in women. The word spontaneous in SCAD, could often convey a potentially erroneous meaning, for the simple reason, plaque ruptures and fissures that triggers dissections of varying lengths can be spontaneous as well.
By the way, any tips to differentiate SCAD from spontaneous plaque ruptures and fissures ?
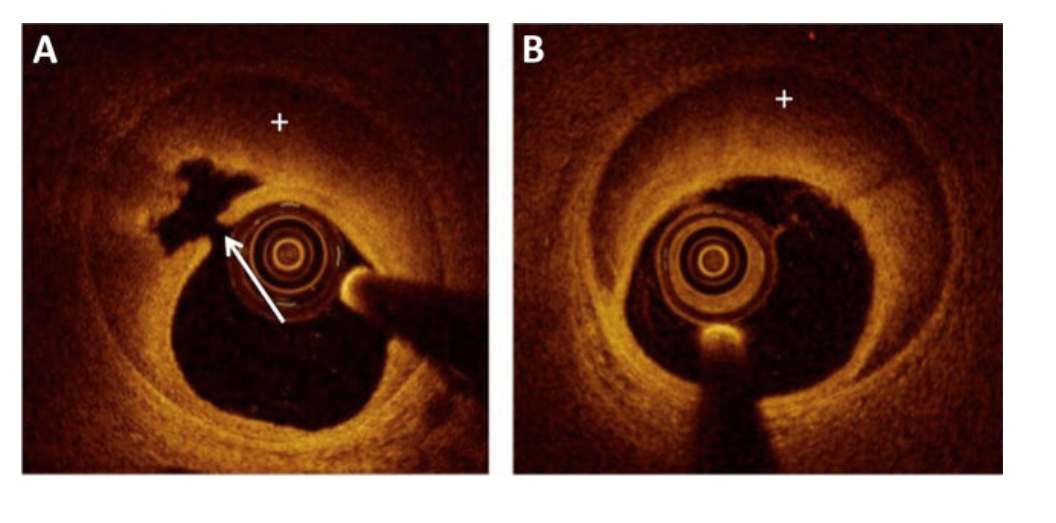
OCT in SCAD : A SCAD caused by an intimal tear (arrow) resulting in expansion of a false lumen and an intramural hematoma (plus sign). B SCAD caused by de novo injury and bleed inside vessel wall resulting in the false lumen with intramural hematoma (plus sign) Source Shah, T et al Curr Cardiol Rep 24, 529–540 (2022). https://doi.org/10.1007/s11886-022-01676-7
Final message
Nothing moves with out a force either from witjin or external . In both SCAD or plaque rupture , an emotional or hemodynamic stress is responsible.
The above list to differentiate SCAD from plaque fissure is big, but few are actually useful. Sometimes, the confirmation comes from the direct feel and the haptics of the lesion and the level of difficulty in crossing the lesion.
Caution : However, in explict clinical situations, as in a young pregnant women with ACS, who has a long spiral dissection , never diagnose anything other than SCAD.
Post-amble: * I wonder, how did the cardiology literature accumulated so much OCT data in SCAD, it should have been very risky procedure in those friable vessels. If PCI is contraindicated , OCT comes very close to it.
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- April 2026 (4)
- March 2026 (9)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,644,793 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

