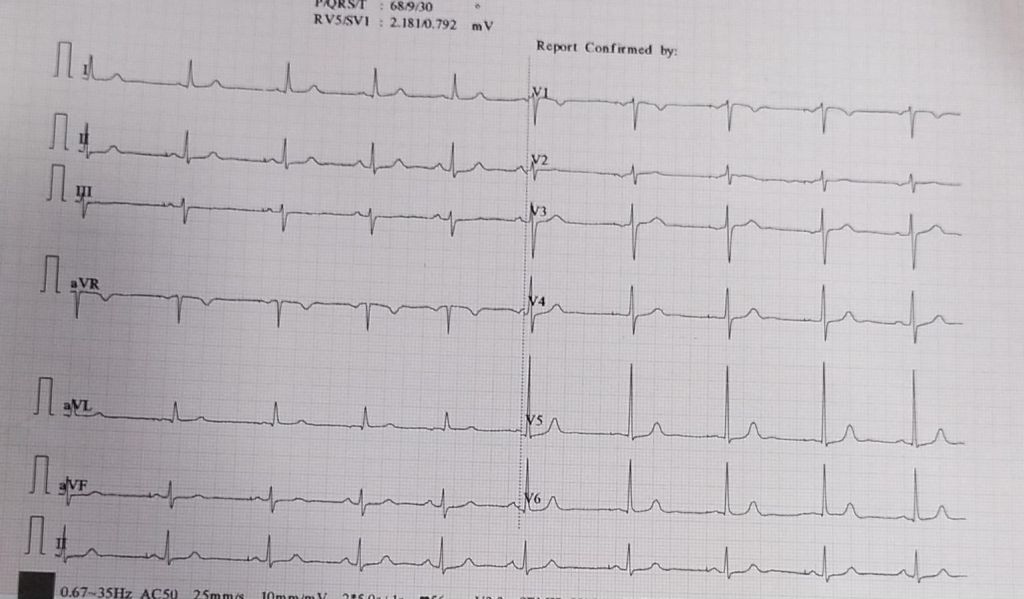
This pateint has
A. Single lead AAI pacemaker
B. DDD in AAI mode* (A pace V sense )
C.Single lead AAIR pacemaker
D. Can never answer this question without X ray or the implantation records.
Answer : I think, we can’t answer this question with this ECG strip. So we can only guess it is DDD, as single chamber AAI pacemaker is not in vogue , even though it is the most physiological pacemaker possible in ideal conditions.( If any one has any points to differentiate , please comment)
* A pace V sense in DDD, though equivalent to AAI mode , can not be compared to AAI pacemaker, for the simple reason, ventricles just don’t have a lead in the later.
Final message
This post might appear as a EP parody. The purpose was different. It is sad to note AAI pacemaker might be dead , but the AAI as a mode will always be a great concept.It can beat on any day , the much hyped LBBBp in bulk of the pateints with SND in terms of physiology and synchrony.Fellows should realise single lead AAI can be most physiological , while, the DDD can become a pathological pacing , if it frequently switches to VVI mode , inspite of good AV conduction.
Part 2 : How do modern day DDD pacemakers reduce ventricle based pacing ?
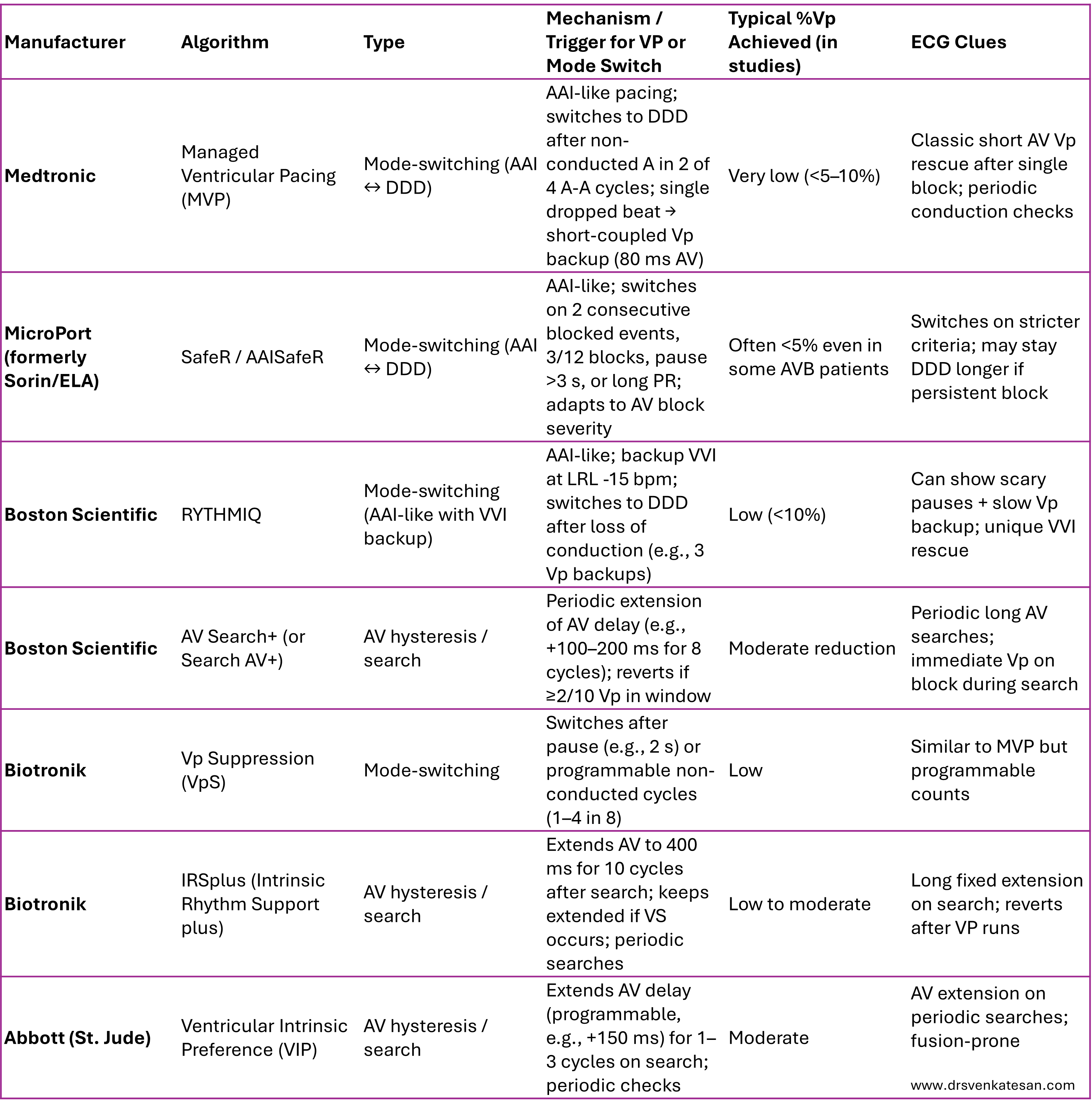
Pacemaker vendors have unique proprietary algorithms designed to minimize unnecessary right ventricular pacing (%Vp) while maintaining atrial-based pacing (effectively mimicking AAI/R behavior) in patients with intact or intermittently preserved AV conduction (e.g., sinus node dysfunction without significant AV block). These algorithms promote intrinsic ventricular activation to avoid dyssynchrony, reduce atrial fibrillation risk, and potentially improve long-term outcomes.
There are two main categories:
- Mode-switching algorithms (AAI(R) ↔ DDD(R)): Operate primarily in atrial-based mode (AAI-like) with ventricular backup; switch to full DDD when AV block criteria are met.
- AV hysteresis / search algorithms: Stay in DDD(R) but dynamically extend the AV delay to search for and favor intrinsic conduction.
Annexure : Company brands and different modes and algorithms (Compiled by Grok)