TAVI is becoming like PCI equivalent of aortic valve. The procedure is nothing but stenting and plastering the aortic prothesis ,with all the native diseased aortic leaflet in-situ. Pre procedure CT aortic valve mapping (rather the entire Aorta) is the key to successful outcome.
While the calcium is the essential bonding force of the valve to the aortic annulus, it can also play some serious spoilsport, along with native leaflet debri . Many times, the hardened calcium are like like sharp 3 dimensional knife hanging over there in root of aorta.
Every TAVI operator has this ligering fear . Will that speck of calcium “ice berg”, hiding 2 mm above the NCC, hit the AV node, when I deploy the valve ? Will the distorted leaflet jump few mm above and hit the coronary ostia , however high it may be. (After all , the exact final landing zone is not determined by the operator , but by the ROC curve)

Every severely calcified valve experiences a Titanic effect , fortunately most valves escape.
Realise how important the accuracy these softwares are .It is just a matter of few mm error . . Apart form calcium distribution pattern , more fundamental parameters like the annular size, shape, and optimal imaging angle are critically important. Here is brief report on various software packages available for pre procedure planning of TAVR.
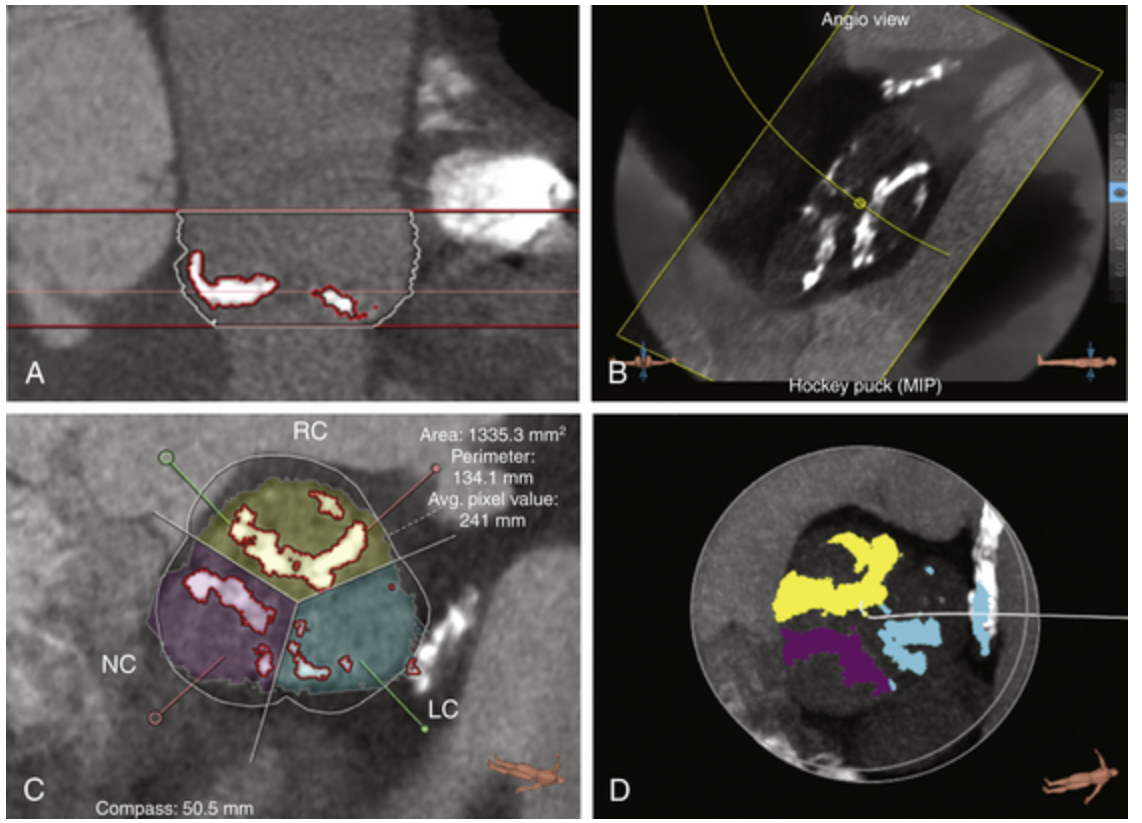
The following table was curated from the respective company websites. Any further details can visit them.
| Software | Vendor/Developer | Key Features for TAVR Pre-Planning |
|---|---|---|
| 3mensio Structural Heart | Pie Medical Imaging | Dedicated TAVR module for automated aortic root analysis, valve sizing, and access route planning. Provides 3D visualization, calcium scoring, and virtual valve implantation. Widely used for precise measurements and procedural simulation. |
| OsiriX MD / Horos | Pixmeo (OsiriX) / Open-source (Horos) | DICOM viewer with 3D multiplanar reconstruction (MPR) tools for manual valve sizing, annulus measurement, and aortic root analysis. Horos is a free alternative. Supports plugins like ProSizeAV for semi-automated sizing. |
| syngo.via CT Cardiac Function – Valve Pilot | Siemens Healthineers | Semi-automated workflow for aortic valve assessment, angulation prediction, and device sizing. Includes valve pilot tools for efficient CT analysis. |
| HeartNavigator | Philips Healthcare | Automated or semi-automated CT processing for TAVR, including aortic root segmentation, access route simulation, and procedural guidance. Often compared for reliability in measurements. |
| Valve Assist 2 | GE Healthcare | AI-assisted tool for valve sizing, CT analysis, and planning efficiency. Focuses on automating measurements to reduce manual effort. |
| Mimics Enlight / Mimics Planner | Materialise | Cloud-based 3D modeling software with automated workflows for structural heart interventions, including TAVR-specific measurements, virtual valve implantation, and 3D printing support. Includes AI for segmentation. |
| cvi42 | Circle Cardiovascular Imaging | Advanced CT tools for interventional planning, including TAVR, with automation for aortic valve assessment, flow quantification, and structural heart disease management. |
| Intuition TAVR Planning | TeraRecon | Comprehensive package for aortic root segmentation, centerline extraction, and pre-operative measurements. Supports advanced 3D/4D visualization for TAVR workflows. |
| Vitrea CT TAVR Planning | Canon Medical (Vital Images) | AI-leveraged application for automated TAVR assessment, including valve sizing, access planning, and post-operative evaluation. Integrates deep learning for efficiency. |
Some questions
1.Which one is most popular ?
With out doubt 3mensio is top software because of its neutrality between various TAVR valve and wide spread usage and comparisons.
2.What is the cost of these software ?
They are substantial has a monthly subscription model. 3Mensio pricing starts at approximately $500/month for 1 user, $4,000/month for 10 users.
3.Is there any Freeware for assessing Aortic root ?
Yes . OsiriX MD / Horos is a free ware, but not getting sufficient attention.
4.What is the error rate of these software ? since they are offline and often images are machine extrapolated ?
Error rate in software are well not reported. (Can’t expect the vendors to do it !) However, It must be acknowledged they are real because of the offline nature of image processing .These tools process DICOM data, in pre-trained algorithms. Errors can arise from poor CT input (e.g., motion artifacts) or extrapolation in 3D reconstruction (e.g., interpolating between slices), but studies show minimal impact with high-quality scans.
Common Error Sources: User variability, calcium blooming artifacts, or phase-specific differences in dynamic CT.
Clinical Implications: Errors in sizing can lead to complications like paravalvular leak (if undersized) or embolism (if oversized), but validation shows risks are low (e.g., <2 mm differences rarely affect outcomes). Multi-reader or expert double check is encouraged to improve accuracy.