Coronary collateral circulation is probably the most poorly understood circulation than any other.This is ignorance at it’s best , in spite of the life saving potential of this circulation. A popular (mis )perception is coronary collaterals can support only resting blood flow and it would struggle to compensate at times of exertion. This is based on few case studies and not based on large , authentic scientific data.
Does this reasoning mean , coronary collaterals can never / ever be complete ?
If we believe so . . .we are grossly underestimating the power of nature .(In fact , mankind was humiliated by the nature time and again !)
Lessons from a unique patient we have encountered.
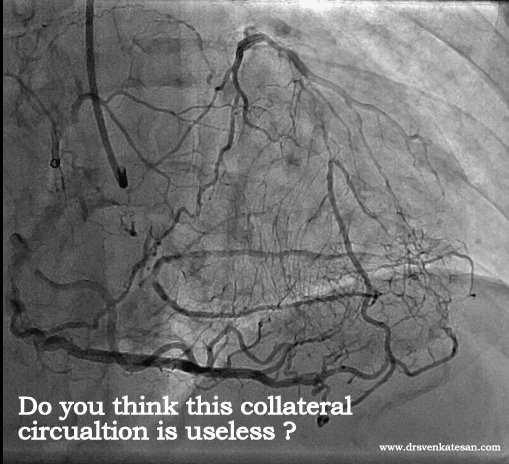
Here is an example of total LAD/LCX occlusion with good collateral from RCA. He was having stable angina on medical management . This patient was not only asymptomatic and was also negative for exercise stress test at moderate work load .

There was an intense debate about the management when this angiogram was presented in the cath meeting .

- Most of the cardiologists believed so ! But they had no answers why his stress test was negative.
- The other argument for CABG was one can not allow a patient with a functionally single coronary artery (RCA) However good is the collateral circulation.This at least has some logic. not the first one !
- One more suggestion was to quantitate and map the real extent of ischemia by PET scanning and then decide about revascularisation.
- One critical opinion was , since he was doing well with medical management what was the need to do coronary angiogram at all ?
Any answers . . .

He ultimately went on to receive CABG (By popular opinion ) , but the point here is the collaterals were good enough to support exertion.We have documented quiet a few similar patients with collateral circulation supporting exercise.
What happened to the collaterals and (of course ) the patient after surgery ?
I will post you the curious story soon . . .
Final message
Coronary collateral circulation , if well developed can provide hemo-dynamically useful support even at times of exertion *
* The existing literature is biased against this concept. It generalizes all grades of collaterals into a single entity. It is better if we spend more time to understand the nuances of coronary collateral circulation .
This is the message from our observation. Do not ever believe whatever is published as facts in scientific literature. Observe, analyse , create your own inference , and concepts. Mainstream cardiologists would brand it unscientific , Simply ignore it . Many times it is rewarding to our patients.




{kind=link}
A myocardial perfusion scan is the next step to assess his myocardial perfusion. Unfortunately this test is underused in India.I would not agree with the statement that he was asymptomatic. He was suffering from stable angina and hence the need for angiogram.At the end of the day, if all the collaterals were supplied by the RCA which is the only patent artery, it only takes a single thrombotic lesion to that artery and his end will be inevitable. So at any cost I think he needs revascularization to the blocked artery. It will be intresting to know what happend follwoing CABG.
Here is an Interesting personal account regarding the collaterals.
Dr. Venkatesan
I’d like to thank you for posting this interesting entry in your blog:
https://drsvenkatesan.wordpress.com/2011/02/03/who-said-coronary-collateral-circulation-can-not-support-excercise/
I am a medical professional from US . I have recently been diagnosed with premature coronary disease – Over the last 20 years of my life, I have not taken good care of myself, and only recently got back into shape. I exercise regularly, aggressively with swimming and compete regularly. In the last month, I have experienced symptoms of angina – only when I reach my maximum heart rate > 175-185. I have no chest pain when I swim with my heart rate monitor at 150-160. I can swim at that rate all day with no problems.
My exercise stress at 15.2 Mets demonstrated no EKG changes, but a Myoview did show an anterior wall perfusion defect. I went on to cardiac cath revealing severe multi vessel disease, most problematic of which was the mid-distal LAD, with near complete occlusion. Interestingly, when the catheter wire tried to traverse the 3 long stenosis, contrast would not pass into the distal LAD as the diameter of the wire essentially occluded the LAD. However, contrast injected into the circumflex backfilled the distal LAD!
My cardiologists and cardiac surgeons believe the collateral flow developed over slow occlusion and exercise has provided enough flow to prevent ischemia in all but the most extreme cases near maximum heart rate.
As there is no bypass that will reach distally to the lesion, I am left with a decision to leave the lesion alone, or move forth with a internal mammary patch angioplasty of the distal LAD.
Again, thank you for the interesting entry.
Signed
Dr. Venkatesan,
I read your blog with great interest and I think I may have something useful to contribute from my own personal experience. I am a 68 year old male with a long history of smoking (for fifty years), and a history of uncorrected hypertension over the years (it has been corrected to normal with medication for many years now). I am a non-smoker now for the past 18 months. I have PAD and a moderate aortic aneurysm of about 3.5CM (ascending and descending) which is being watched with regular vascular scans.
The common femoral arteries in both of my legs are nearly 100% occluded between my thighs and my knees, and yet my ankle and toe blood pressures (and my circulation in my ankles and feet) is almost normal. The reason for that is that according to the vascular scan, my deep femoral arteries are much larger caliber than normal with extensive vascular collateralization by passing the common femoral occlusions.
About twenty years ago before the PAD diagnosis, I realized that I had claudication in both of my calves when I walked a short distance. I expected this was being caused by an arterial blockage in my legs, so I went to the gym every day for about three years, and walked through the pain every day. I believe this contributed to the formation of the collaterals that have perhaps saved my legs and feet.
I also have heart disease, and had a fairly minor heart attack in 1999. No stents were placed nor angioplasty performed at that time. I recently had an arteriogram and cardiac stress MRI which showed that two of the three coronary arteries are now 100% occluded (apparently I had another cardiac event and did not know it). The cardiologist says that the LAD is in extremely good condition and has numerous collaterals branching from it. I have no symptoms whatever from all of this, except that my LVEF is low (about 35%). I walk at a very brisk pace six miles per day, five days per week, and I monitor my pulse rate with a pulse monitor when I walk. I keep my pulse between 115 and 120 which I calculate to be 80% of maximum for my age. I believe this cardio exercise / walking has also helped with the collateral formation, and I am hoping to bring the LVEF back up to a reasonable number with this exercise regimen.
My cardiologist has recommended an ICD, but I have decided against that since I have never had VT or VF or any other type of cardiac arrythmia (except for non-symptomatic PVC’s which I was born with).
I believe that I am the lucky recipient of good genetics to begin with, but also I am highly motivated now to take better care of myself, and know as much as I can about the conditions that I have. I plan to have an echocardiogram in six months to see if the LVEF numbers have improved, and I fully expect that they will have. I give credit to the smoking history for the vascular problems that I have including the cardiac problems. I am a lucky person I think, and suspect that not everyone has the fortunate ability to heal themselves the way I have.
I have asked for copies of my arteriogram and stress MRI records. If you are interested in looking at these I would be happy to share them with you.
Dear Mr Weigel
Yours is an extremely interesting story told in a most scientific manner.Thank you .
It gives me great insight , how a human vascular system can transform when confronted with natural disasters like multiple blocks on its way .A flowing river will definitely reach its destination however bizarre the path it takes . Human biology is vested with vast reserves of genetic building blocks put on sleep mode. While billions of dollars are being pumped into do research in human angiogenesis we have tuned a blind eye to the vast net work of natural collaterals.
Our clinical experiences also tell the same thing . In chronic total occlusion majority of patients would develop good collaterals if only we do not tamper the main vessel .None of scientific studied available has proven opening CTOs (Chronic total occlusions) has improved the clinical outcome .
Regarding the guidelines for revascualrisation , I am yet to come across a standard scientific guidelines that includes the extent of collateral circulation as one of the determinant for need for revascularisation !
I will definitely use your case study for the benefit of so many patients ! I always feel , a properly interpreted experience , even from a single patient can make a tremendous impact in the growth of science .
Thanks again for sharing your personal health issues !
Dr Venkatesan
Chennai .India .
[…] be eye opener for others , I am jut posting it here . The comment was in response to my article Who said coronary collateral circulation will not support exercise ? here is the […]
Hi there Pete a hard core blue collar guy in virginia did alot of scaffolding 100 to 300 feet tall. So the work was beyond strenous. Well I had a 90% blockage stented but there is a 100% blocked one they said has been blocked for years and I grew 2 laterals. Then thats it told me to see how things go. hmmmm thank God I worked my butt off over the years now I understand I have to work and exercise as if Im 25 years old again Im 48 years old now.
Dear Sir,
Really pertinent observation that large collaterals can more than adequately support the territory after a CTO, often making us rethink whether any revascularisation is warranted at all. Myocardial perfusion imaging at peak stress may be the way to decide, finally. Thanks for a great article.
Anxious to know what happened to the patient after the CABG?
Dr Venkatesan,This is very Informative and I appreciate your blog from core of my heart and I have a similar story to share .. On 28 Jan 17 I visited cardiologist for a routine TMT after 10 years and it was found +ve which says ST depression -3.75mm in III at 8:56min depression change -3.57mm in v5 07:05min but I never had any angina . Later on angiogram found 100% stenosis after LAD diagonal1 supported by collaterals from RCA & PDA,Distal LCx 90% long stenosis OM1 -mid segment has 90% stenosis,PDA has diffuse 90%stenosis ,PLV has 90% long proximal stenosis . My stenting failed in LAD as blocks are calcified and I ignored bypass option till I develop some kind of angina . However I am taking lots of medicines as per medical advise and walk 50000 steps every week . I take vegitarian non oily and no diary diet . I shall be looking more towards your blog to get feedbacks on Myocardial perfusion imaging so that I can assess my heart periodically
Hi Doctor Venkatesan,
Just want to know is there a way to encourage more collateral arteries to grow? I had 5 stents for not even having a heart attack or chest pain or even shortness of breath. My doctor in Japan told me I needed 5 long stents in my RCA and LAD. Now, I feel worst in my life everyday. I have shortness of breath and chest discomfort everyday 24/7. I was thinking I probably had enough collateral arteries that is why I never had any symptoms before my angioplasty and stenting. The doctor asked me to have a recheck after 1 year but I refused as I know they will put more stents in me for the money and, it will speed up my death. I thought if I’m going to die anyway soon, why have a recheck, put more stents and die quicker??